Ovulation Tests: How They Work, When to Use Them, and What Your Results Mean
A fertility nutritionist's guide to ovulation predictor kits — how they detect LH, when to test, what your results mean, and which type is worth your money.


If you've spent any time trying to conceive, you've probably stared at a little plastic stick wondering whether the second line is dark enough. It's one of those small rituals that define the early stages of the fertility journey — peeing on a stick, squinting under the bathroom light, checking again twenty seconds later. Welcome to the world of ovulation tests — also known as ovulation predictor kits, or OPKs.
I recommend ovulation tests to nearly all my clients who are actively trying to get pregnant. They're cheap, they're easy, and they give you something more useful than any fertility app can: a real-time signal from your actual body — tied to where you are in your menstrual cycle — not a calendar estimate. But they come with nuances that most packaging doesn't explain — and getting those details right can genuinely affect your timing.
Here's everything I want you to know about how ovulation tests work, when to use them, and what your results actually mean.
Key Takeaways
- Ovulation tests measure LH in your urine — a surge means ovulation is likely within 24–36 hours
- Cheap strip tests are just as accurate as digital ones (Vanderhoff et al., 2024 found 92–97% accuracy across five brands)
- Start testing around day 10 of a 28-day cycle, or your cycle length minus 17
- Test between 10am and 8pm with concentrated urine — not first morning urine
- A positive test doesn't confirm you've ovulated, only that your body is preparing to — combine with BBT or cervical mucus for confirmation
What Ovulation Tests Actually Measure
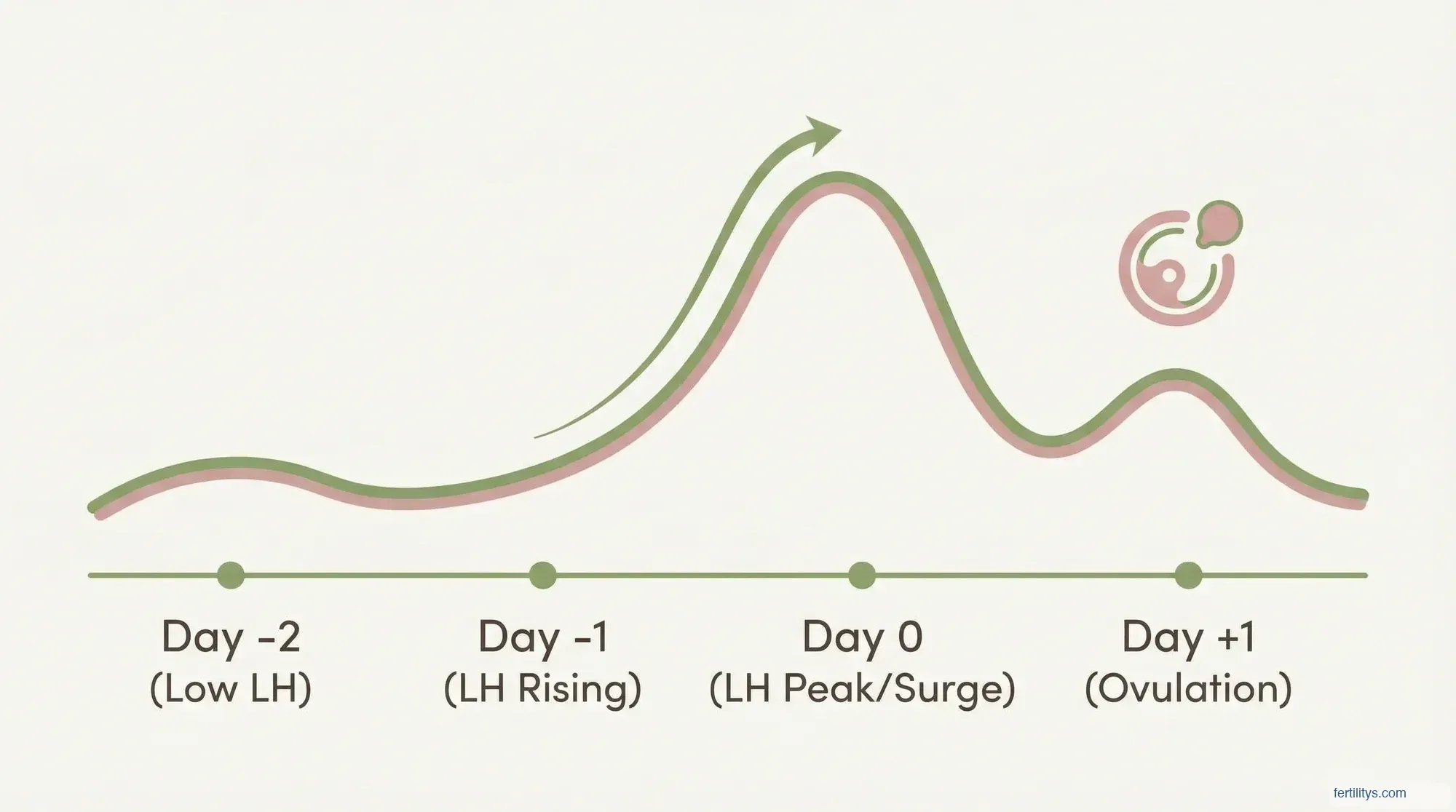
Every month — assuming you're ovulating regularly — your brain sends a hormonal signal to your ovaries that it's time to release an egg. That signal is a rapid rise in luteinising hormone, commonly called the LH surge.
LH is produced by your pituitary gland throughout your cycle, but it spikes dramatically about 24–36 hours before ovulation. A meta-analysis by Park et al. (2022) across six studies and 187 cycles found the mean time from LH surge onset to ovulation was 33.9 hours (95% CI: 30.8–37.0). That spike is what ovulation tests detect.
The test strip contains antibodies specific to LH. When you dip it in urine (or hold it in your stream, depending on the brand), LH binds to those antibodies and produces a visible line. The darker the line relative to the control, the higher your LH concentration.
What triggers the LH surge in the first place? As your dominant follicle grows during the follicular phase, it produces rising levels of oestrogen. Once oestrogen hits a certain threshold, it flips from suppressing LH to triggering a sudden release — the surge. This is the same oestrogen rise you might notice as increased cervical mucus or a more upbeat mood mid-cycle.
How to Use an Ovulation Test (Step by Step)
The instructions on the box are usually fine for the basics, but there are details they don't always mention. Here's how I walk my clients through it:
When to start testing. Take your usual cycle length and subtract 17. That's roughly the day to begin. For a 28-day cycle, that's day 11. For a 32-day cycle, start on day 15. If your cycles are irregular, start testing from day 8 or 9 to avoid missing your surge entirely.
What time of day. This is where most guides get it wrong. Unlike pregnancy tests, ovulation tests are best taken between 10am and 8pm — not with your first morning urine. Su et al. (2017) found the LH surge onset primarily occurs between midnight and early morning (37% between midnight and 4am), which means it often won't appear in urine until later that day. Test with urine that's been held for at least two hours without excessive fluids.
Reading the result. A positive ovulation test means the test line is as dark as or darker than the control line. Unlike a pregnancy test, where any faint line is a positive, ovulation strips need that equal-or-darker threshold. A faint line just means LH is present at baseline levels — which it always is.
Once you see a positive: have sex that day and the following day. Your egg, once released, only survives about 12–24 hours. But sperm can live up to five days in the reproductive tract, so having sex before ovulation actually gives better odds than waiting until after. More on timing in my preconception guide.
Strip Tests vs. Digital Ovulation Tests: Is One Better?
I get asked this constantly. The short answer: both work. The longer answer is a bit more interesting.
Basic strip tests (Easy@Home, Wondfo, Pregmate) cost around £0.20–£0.50 per strip. They show two lines — you compare the darkness yourself. A 2024 study by Vanderhoff et al. in Fertility and Sterility compared five popular OPK brands against blood LH levels and found accuracy ranged from 91.75% to 96.90%, with the cheaper strips (Pregmate at 96.90%, Easy@Home at 95.88%) actually performing slightly better than Clearblue (91.75%).
Digital ovulation tests (like Clearblue Digital or Clearblue Advanced) give a clear smiley face or circle — no line comparison needed. The Advanced version also measures oestrogen alongside LH, which can identify your "high fertility" days before the peak. That wider window can be helpful if you want more advance notice.
My honest take? Start with the cheap strips. A 50-pack of Easy@Home costs around £8–£12 and gives you enough for several cycles of testing. If you find line comparison stressful or your cycles are unpredictable, a digital test removes the ambiguity. But don't pay ten times more thinking you're getting ten times more accuracy — the research says you aren't.
What Your Results Mean (and What They Don't)
A positive ovulation test tells you one specific thing: your LH has surged. That's it. What it doesn't tell you is whether ovulation will definitely follow.
LH surge without ovulation. This can happen. A follicle may start to mature, trigger an LH surge, but then fail to release the egg — a condition sometimes called luteinised unruptured follicle syndrome (LUFS). It's more common than you'd think: some estimates suggest it occurs in up to 10% of natural cycles. If you're getting positive OPKs but not conceiving after several months, this is worth investigating with your GP.
Consistently faint lines or always negative. If your tests never show a clear positive, a few things could be happening. You might be testing at the wrong time of day, your surge could be very short (some women surge for only 12 hours — easy to miss with once-daily testing), or you may not be ovulating regularly. Anovulation is more common than most people realise, particularly with PCOS, stress, undereating, or excessive exercise.
Multiple positives in a row. Some women see dark lines for three or four days straight. This is usually normal — LH doesn't just spike and vanish; it rises, peaks, and then falls. Ovulation typically happens after the first positive test, not the last. Time sex from that first positive.
PCOS and false positives. If you have polycystic ovary syndrome, your baseline LH levels may be chronically elevated — meaning OPKs can show a positive result even when you're not actually surging. Women with PCOS often have an LH-to-FSH ratio of 2:1 or higher, which can make standard strip tests unreliable. If this sounds like you, consider a quantitative hormone monitor that tracks actual LH values rather than a simple threshold, or work with your GP to confirm ovulation via progesterone blood tests.
Ovulation Tests vs. Other Tracking Methods
OPKs aren't the only way to track your cycle, and they work best when combined with other signals. Here's how they compare:
Basal body temperature (BBT) confirms ovulation after it's happened — your temperature rises by about 0.2°C following the progesterone surge post-ovulation. It's retrospective, so it won't help you time sex in the current cycle, but over a few months it shows your pattern. Used together with OPKs, you get both the prediction and the confirmation.
Cervical mucus is remarkably reliable once you know what to look for. Fertile mucus (stretchy, clear, egg-white consistency) appears in the days leading up to ovulation as oestrogen rises. It's free, it's always available, and it often gives you a wider warning window than an LH test. I teach all my clients to check mucus alongside using OPKs — it's one of the oldest tracking methods and still one of the best.
Cycle-tracking apps predict ovulation based on your past cycle lengths, but a study by Johnson et al. (2018) found that calendar-based predictions alone cannot accurately pinpoint ovulation day because it varies considerably even in regular cycles. Apps are useful for logging data, but don't rely on them as your sole predictor — use them to record your OPK results and BBT readings instead.
The gold standard? OPK + cervical mucus + BBT. The three together give you advance warning, real-time confirmation, and retrospective proof. If that feels like too much, start with OPKs and cervical mucus — that combination catches most of what you need.
For a more detailed breakdown of your fertile days, try our ovulation calculator.
Common Mistakes That Skew Your Results
Testing with first morning urine. I know pregnancy tests say to use it, but ovulation tests are different. LH synthesised overnight may not have filtered into urine yet by morning. Afternoon or early evening testing — with a two-hour hold — catches the surge more reliably.
Drinking too much water beforehand. Over-hydration dilutes your urine and can wash out the LH signal entirely. Reduce fluids for a couple of hours before testing.
Reading results too late. Most strip tests need to be read within five minutes. After that, evaporation lines can appear and make a negative look positive. Set a timer.
Only testing once a day. If your LH surge is short (under 24 hours), once-daily testing can miss it completely. If you've had several cycles with no positive result, try testing twice daily — once around noon and once in the early evening.
Stopping too soon after a positive. Some women test, see a positive, and stop. Keep testing for another day or two after the first positive. This helps you understand your surge pattern — is it a one-day spike or a gradual two-day rise? That information becomes useful over multiple cycles.
When Ovulation Tests Might Not Be Right for You
OPKs are brilliant tools, but they're not perfect for everyone.
If you have PCOS, the elevated baseline LH I mentioned earlier can make standard strip tests unreliable. You may need to combine OPKs with ultrasound monitoring or use a quantitative monitor like Inito that tracks actual hormone levels.
If you're taking fertility medications — particularly those containing hCG (like trigger shots) or LH — your test results will be affected. hCG is structurally similar to LH, so it can trigger a false positive. Ask your clinic how to interpret OPK results alongside your medication protocol.
If your cycles are extremely irregular (varying by more than 7–10 days), you might use a lot of test strips each cycle trying to catch the surge. A fertility assessment with your GP might be a more efficient starting point to understand what's happening with your cycles before investing in months of testing.
If tracking is increasing your anxiety, it's OK to step back. I've worked with women who found the daily testing ritual turned sex into a chore and trying to conceive into a medical procedure. If that's where you are, take a break. Your body is still ovulating whether you test or not.
The Bottom Line
Ovulation tests are one of the simplest, most accessible tools you have for understanding your fertile window. They won't guarantee pregnancy — nothing can — but they take the guesswork out of timing, and timing genuinely matters when it comes to your chance of getting pregnant. Wilcox et al. (1995) showed in the New England Journal of Medicine that the probability of conception drops to nearly zero outside the six-day fertile window, with peak chances on the day before and the day of ovulation.
Start with affordable test strips, test in the afternoon with a two-hour hold, and pair your results with at least one other tracking method. And if several months of positive OPKs haven't led to a positive pregnancy test, have a conversation with your GP. There's no shame in asking for help — and there's often a straightforward next step they can offer.
▸Can ovulation tests detect pregnancy?
Technically, yes — but not reliably. LH and hCG are structurally similar, so a very sensitive OPK may show a positive if you're pregnant. But ovulation tests aren't designed or calibrated for pregnancy detection. Always use a dedicated pregnancy test instead.
▸How long after a positive ovulation test do you actually ovulate?
Most research puts it at 24–36 hours after the surge begins, with a meta-analysis averaging 33.9 hours. But this varies — some women ovulate within 12 hours, others take up to 48. This is why having sex on the day of the positive test and the day after gives you the best coverage.
▸Are ovulation tests accurate for women with PCOS?
They can be unreliable. PCOS often causes chronically elevated LH, which means you may get frequent false positives. If you have PCOS, consider combining OPKs with basal body temperature or using a quantitative monitor that tracks actual hormone concentrations rather than a simple positive/negative threshold.
▸Is it better to test in the morning or evening?
Between 10am and 8pm is ideal. The LH surge often begins in the early morning hours, and it takes several hours for the hormone to appear in detectable concentrations in urine. Testing with concentrated afternoon urine (after a two-hour hold) gives the most reliable results.
▸Do ovulation tests confirm that ovulation has happened?
No. An OPK confirms your LH has surged — it predicts ovulation but doesn't verify it occurred. To confirm ovulation, you need either a progesterone blood test taken 7 days after the expected ovulation, a sustained BBT rise, or ultrasound monitoring. A positive OPK followed by a BBT shift is a strong indicator, though.
You might also find helpful:
References
- Park SJ, Goldsmith LT, Skurnick JH, et al. "The LH surge and ovulation re-visited: a systematic review and meta-analysis." Human Reproduction Update. 2022;28(4):554-567. doi:10.1093/humupd/dmac010
- Vanderhoff AC, Liberman A, Walling I, Ginsburg ES. "Similar accuracy and patient experience with different one-step ovulation predictor kits." Fertility and Sterility. 2025;123(3):499-505. doi:10.1016/j.fertnstert.2024.09.031
- Su HW, Yi YC, Wei TY, Chang TC, Cheng CM. "Detection of ovulation, a review of currently available methods." Bioengineering & Translational Medicine. 2017;2(3):238-246. doi:10.1002/btm2.10058
- Wilcox AJ, Weinberg CR, Baird DD. "Timing of sexual intercourse in relation to ovulation — effects on the probability of conception, survival of the pregnancy, and sex of the baby." New England Journal of Medicine. 1995;333(23):1517-1521. doi:10.1056/NEJM199512073332301
- Johnson S, Marriott L, Zinaman M. "Can apps and calendar methods predict ovulation with accuracy?" Current Medical Research and Opinion. 2018;34(9):1587-1594. doi:10.1080/03007995.2018.1475348
- Ecochard R, Duterque O, Leiva R, et al. "Self-identification of the clinical fertile window and the ovulation period." Fertility and Sterility. 2015;103(5):1319-1325. doi:10.1016/j.fertnstert.2015.01.031
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making decisions about your fertility, cycle tracking, or conception strategy. I'm a registered nutritionist (MSc, RNutr), not a medical doctor.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











