Folate and Fertility: What It Does, Why You Need It, and Which Form to Take
Folate is one of the most important nutrients for fertility — but should you take folic acid or methylfolate? A registered nutritionist explains the science, the doses, and which form works best.


If there's one supplement I'm asked about more than any other, it's folate. Or folic acid. Or methylfolate. And that confusion — right there — is actually part of the problem.
Most women know they should take folic acid when they're pregnant. The NHS says so, the midwife says so, the packet on the shelf at Boots says so. But what fewer people realise is that folate does far more than prevent neural tube defects — and that the form you take might matter just as much as whether you take it at all.
I'm a registered nutritionist who specialises in fertility, and folate was a cornerstone of the protocol I built for myself when my AMH came back at 3. It's one of the first things I look at with every client. So let me walk you through what folate actually is, why it matters for conception, and how to make sure you're getting enough — in the right form.
📋 Key Takeaways
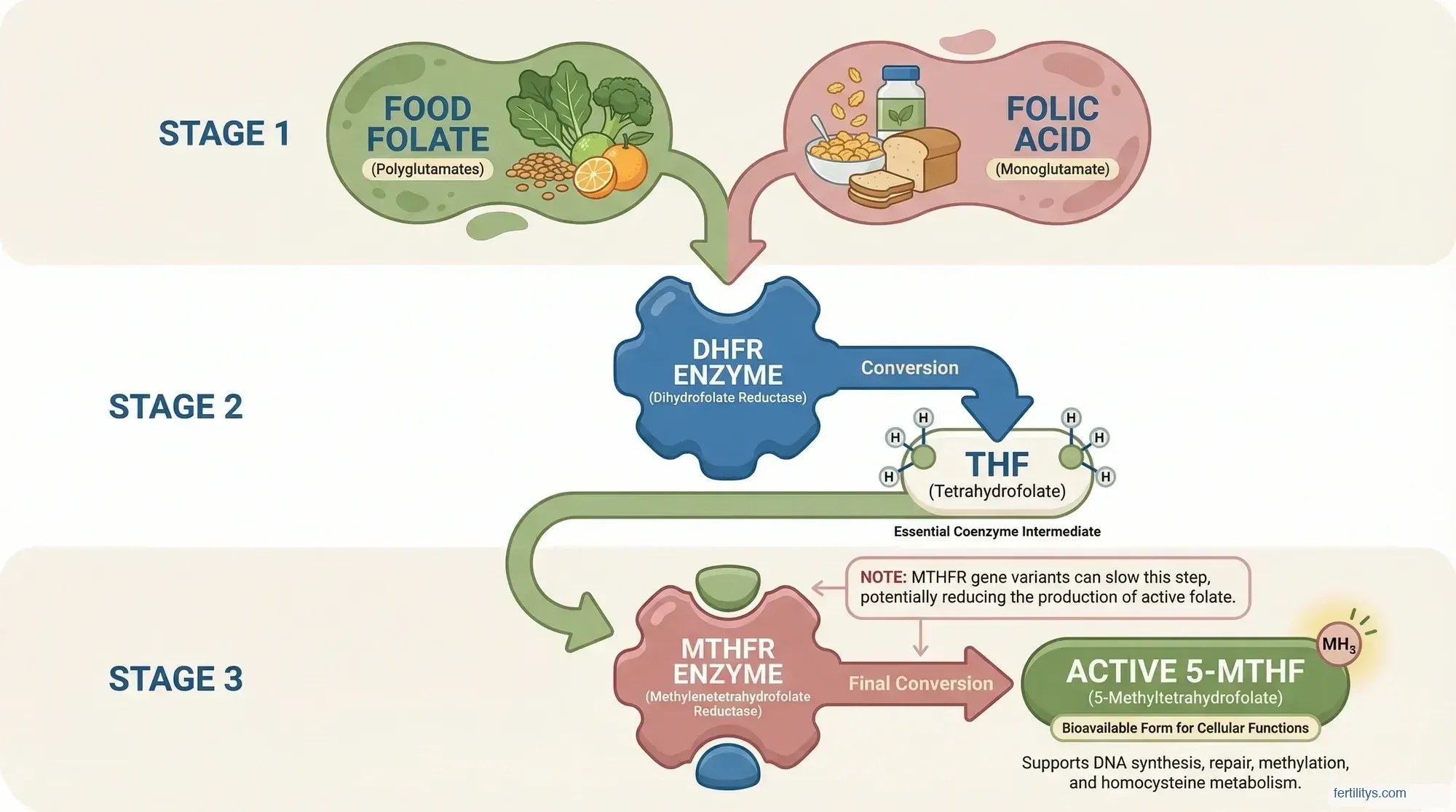
- Folate and folic acid aren't the same thing. Folate occurs naturally in food; folic acid is synthetic. Both need to be converted to the active form (5-MTHF) before your body can use them.
- Around 40% of people carry an MTHFR gene variant that makes converting folic acid harder — methylfolate bypasses this entirely.
- 400mcg daily is the minimum. The UK NHS, WHO, and US Preventive Services Task Force all recommend at least 400mcg before conception and through the first 12 weeks.
- Start at least 3 months before trying to conceive — I recommend a year where possible, because egg maturation takes roughly 90 days and you want folate levels optimised well before that window.
- Food sources matter too. Dark leafy greens, lentils, chickpeas, asparagus, and broccoli are some of the richest natural sources.
What Folate Actually Is — And Why It's Not the Same as Folic Acid
Folate is vitamin B9 — one of the eight B vitamins your body depends on for energy, brain function, and cell division. It's a water-soluble vitamin that your body can't make on its own, so you have to get it from food or supplements. It's involved in DNA replication, amino acid metabolism, red blood cell production, and the creation of new cells — which makes it absolutely fundamental to reproduction.
Folate deficiency is more common than most people realise. In the UK, a government population survey found that the average dietary folate intake for women was just 250mcg per day — below the recommended 300mcg, and well below what you need during preconception. Severe folate deficiency can cause folate deficiency anaemia, where your body produces abnormally large red blood cells that can't function properly. Symptoms include fatigue, weakness, and breathlessness — none of which help when you're trying to conceive.
Here's where the terminology gets messy. Folate is the natural form of folate found in food — spinach, lentils, asparagus, broccoli. Folic acid is a synthetic version created in the 1940s, used in folic acid supplements and fortified foods like breakfast cereals and bread. Neither one is biologically active on its own. Both need to be converted into a form called 5-methyltetrahydrofolate (5-MTHF), which is the form that actually circulates in your blood and does the work.
The conversion process matters. Your body handles food folate and synthetic folic acid differently. Food folate is absorbed at roughly 50% bioavailability. Folic acid from supplements is absorbed at around 85% — higher, yes, but it has to go through a multi-step enzymatic process to become 5-MTHF. And for a significant chunk of the population, that conversion doesn't work properly. More on that in a moment.
This distinction isn't academic. When I sit down with a new client and look at what supplements they're taking, I always check which form of folate is in their prenatal. It makes a real difference. I also check their vitamin B12 status alongside folate — the two work together closely, and a vitamin B12 deficiency can mask or mimic folate deficiency symptoms, which complicates the picture.
Why Folate Matters for Fertility — Before, During, and After Conception
You probably already know folate prevents neural tube defects (NTDs) like spina bifida. The WHO, the NHS, and the US Preventive Services Task Force all agree on this — it's one of the most well-evidenced findings in maternal nutrition. The landmark MRC Vitamin Study (1991) demonstrated that folic acid supplementation reduced NTD recurrence by 72%, and that finding reshaped public health policy worldwide.
But folate does much more than protect the neural tube. Here's what the research shows:
DNA replication and egg quality. Every time a cell divides — which is happening constantly during egg maturation, fertilisation, and early embryo development — it needs folate for accurate DNA copying. Greenberg et al. (2011) in Reviews in Obstetrics and Gynecology noted that folate is required for purine and pyrimidine synthesis during DNA and RNA assembly. Poor folate status means more DNA replication errors, which can affect egg quality and embryo viability.
Homocysteine regulation. Folate helps convert homocysteine (an amino acid) into methionine. When folate is low, homocysteine builds up — and elevated homocysteine has been linked to recurrent miscarriage, pregnancy loss, pre-eclampsia, and placental abruption. I had two chemical pregnancies myself, and while I'll never know the exact cause, optimising my folate status was one of the first things I addressed.
Conception rates. A secondary analysis from the 2002 Hungarian NTD randomised controlled trial found that women taking a multivitamin containing 800mcg of folic acid had higher conception rates compared to the placebo group — suggesting folate supports fertility beyond just NTD prevention.
IVF and assisted reproduction. Gaskins et al. (2014) published in Obstetrics & Gynecology that among women undergoing IVF, higher folate intake was associated with better outcomes — including higher live birth rates. The EARTH study (Environment and Reproductive Health) of 232 women found that those with the highest supplemental folate intake had significantly higher rates of implantation and live birth.
The MTHFR Question: Do You Need Methylfolate?
This is where it gets genuinely important, and where I think too many women are being let down.
MTHFR stands for methylenetetrahydrofolate reductase — it's the enzyme that converts folate into its active form (5-MTHF). About 40% of the global population carry a variant in the MTHFR gene that reduces how efficiently this enzyme works. The two most studied variants are C677T and A1298C.
If you're homozygous for C677T (meaning you carry two copies of the variant), your MTHFR enzyme activity can be reduced by up to 70%. That means even if you're taking folic acid every day, your body may struggle to convert it into the form it can actually use. The result? Unmetabolised folic acid (UMFA) building up in your blood, while your cells are still short of active folate.
Cueto et al. (2022) reviewed the evidence and concluded that 5-MTHF is a better option than folic acid for correcting metabolic defects in gametes and embryos — particularly for people with MTHFR variants. Servy et al. documented cases of couples with repeated miscarriages and failed IVF cycles who achieved pregnancy after switching from folic acid to 5-MTHF.
Now, I want to be balanced here. The CDC still states that 400mcg of folic acid daily can increase blood folate levels regardless of MTHFR genotype. And they're not wrong — for many people with milder MTHFR variants, standard folic acid is enough. But if you've had unexplained infertility, recurrent losses, or know you carry the C677T variant, methylfolate is worth discussing with your doctor or nutritionist.
I personally use methylfolate. When I was building my protocol, I chose a prenatal containing 5-MTHF rather than folic acid — my Wild Nutrition supplement uses the active form. It was one of those decisions where the potential benefit clearly outweighed any downside, especially given that methylfolate has no known disadvantages compared to folic acid.
How Much Folate Do You Need?
The recommendations are broadly consistent across the UK and US, though the fine print differs:
UK (NHS / NICE): 400mcg folic acid daily from the time you start trying to conceive until at least week 12 of pregnancy. If you have a history of NTDs, diabetes, coeliac disease, or take anti-epileptic medication, the dose increases to 5mg daily (prescription only).
US (USPSTF, updated 2023): 400–800mcg folic acid daily for all women planning or capable of pregnancy. The 2023 USPSTF evidence review, published in JAMA, reaffirmed this recommendation with a Grade A rating — their highest level of certainty.
WHO: 400mcg daily from the moment you begin trying to conceive through the first 12 weeks of pregnancy.
My recommendation? Start earlier than "when you begin trying." Egg maturation takes roughly 90 days, so the folate levels in your body three months before conception directly influence the quality of the egg that gets fertilised. I tell my clients to start at least 3 months before — and ideally a year, because it gives you time to build up stores, identify any absorption issues, and optimise your wider nutrition alongside folate.
The standard dose of folic acid — or methylfolate — is 400mcg daily. Some practitioners recommend higher doses (600–1,000mcg) for women with known MTHFR variants, but this should be guided by a healthcare professional. The amount of folate you need also depends on factors like whether you're taking medications that interfere with absorption (like methotrexate or certain anti-epileptics) and how much folate you're already getting from your diet.
The Best Food Sources of Folate
Supplements are important, but I always come back to food first. Your body absorbs food folate differently — it comes packaged with cofactors, fibre, and other nutrients that support absorption and utilisation. The bioavailability of food folate is lower than synthetic folic acid (roughly 50% versus 85%), but the nutritional context matters.
Here are some of the good sources of folate, based on data from the NIH Office of Dietary Supplements:
- Dark leafy greens: Spinach (131mcg per 100g cooked), kale, Swiss chard, collard greens
- Legumes: Lentils (181mcg per 100g cooked), chickpeas, black beans, edamame
- Asparagus: 149mcg per 100g cooked — one of the highest vegetable sources
- Broccoli and Brussels sprouts: 108mcg and 78mcg per 100g cooked
- Beetroot: 80mcg per 100g cooked (the greens are even richer)
- Avocado: 81mcg per whole avocado
- Eggs: 47mcg per large egg (concentrated in the yolk)
- Citrus fruits: One medium orange provides about 40mcg
One thing to be aware of: cooking destroys up to 90% of natural folate in some foods. Steaming is gentler than boiling, and eating some raw greens (in salads or smoothies) preserves more. This is one reason I'm such an advocate for adding raw spinach to morning smoothies — it's an easy, consistent way to boost your daily intake.
🍎 Go Organic With the Dirty Dozen
These twelve fruits and vegetables carry the heaviest pesticide loads. I tell all my clients: if you can only afford to go organic on some things, make it these. The rest you can buy conventional and wash well.
The list: Strawberries, spinach, kale/collard/mustard greens, peaches, pears, nectarines, apples, grapes, bell & hot peppers, cherries, blueberries, green beans (EWG, 2025).
Folate and Male Fertility
Folate isn't just a women's nutrient. Sperm cells divide rapidly during spermatogenesis — the whole process takes about 74 days — and folate is needed for that DNA replication just as much as it is for egg maturation.
The evidence here is genuinely mixed, and I want to be honest about that. Boxmeer et al. found an inverse correlation between seminal plasma folate concentration and sperm DNA fragmentation in fertile men — meaning higher folate, less DNA damage. And some RCTs have shown folate supplements increase sperm concentration and motility.
But the largest trial to date — the FAZST trial (Schisterman et al., 2020, published in JAMA) — found no improvement in semen quality or live birth rates when men took folic acid plus zinc compared to placebo. The supplemented group actually had higher DNA fragmentation rates (29.7% vs 27.2%). That's a concerning finding, though it's worth noting the study used folic acid specifically, not methylfolate, and didn't account for MTHFR status.
My take: the evidence doesn't support mega-dosing folic acid for male fertility the way it does for women. But ensuring adequate folate intake through diet — plenty of leafy greens, legumes, whole grains — is sensible for any man who's trying to conceive. If your partner takes a male prenatal or fertility supplement, check whether it contains methylfolate rather than folic acid.

The Bottom Line
Folate is one of the most well-researched nutrients in reproductive health, and for good reason. It's essential for DNA replication, it protects against neural tube defects, it regulates homocysteine, and it supports egg and embryo quality. The evidence for supplementing before conception is overwhelming — this isn't a "nice to have," it's a genuine non-negotiable if you're planning a pregnancy.
Where things get more nuanced is the form you take. For most people, standard folic acid at 400mcg daily will do the job. But if you carry an MTHFR variant — or if you've experienced unexplained losses or failed fertility treatment — methylfolate (5-MTHF) bypasses the conversion bottleneck entirely and is worth considering.
And don't forget the food. A folate-rich diet built around dark leafy greens, lentils, beans, and asparagus doesn't just provide B9 — it provides the complete nutritional context that supports absorption and long-term fertility. Supplements fill the gap; food builds the foundation.
▸Is folate the same as folic acid?
No. Folate is the natural form of vitamin B9 found in foods like spinach, lentils, and asparagus. Folic acid is the synthetic version used in supplements and fortified foods. Both must be converted to 5-methyltetrahydrofolate (5-MTHF) before your body can use them, but the conversion pathways differ — and some people convert folic acid less efficiently due to MTHFR gene variants.
▸When should I start taking folate if I'm trying to conceive?
At least 3 months before you start trying, though I recommend a year where possible. Egg maturation takes roughly 90 days, so the folate circulating in your body today influences the quality of eggs maturing right now. Starting early gives you time to build optimal blood levels and address any absorption issues.
▸Should I take methylfolate instead of folic acid?
If you know you carry an MTHFR gene variant (especially C677T homozygous), methylfolate (5-MTHF) bypasses the conversion step that your body struggles with. For everyone else, standard folic acid at 400mcg is generally sufficient. There's no disadvantage to choosing methylfolate — it works for everyone — so many fertility practitioners now recommend it as the default.
▸Can I get enough folate from food alone?
It's difficult. The recommended daily intake for preconception is 400mcg from supplements on top of dietary folate. Food folate has roughly 50% bioavailability compared to supplements, and cooking destroys up to 90% in some foods. A folate-rich diet is important for your broader nutritional foundation, but most health organisations recommend a supplement as well — especially before and during early pregnancy.
▸Does my partner need folate too?
Folate supports DNA replication during sperm production, and some studies show higher folate levels are associated with lower sperm DNA fragmentation. However, the largest trial (FAZST, 2020) didn't find that folic acid supplements improved fertility outcomes in men. Ensuring adequate folate through diet — leafy greens, legumes, whole grains — is sensible, but mega-dosing isn't supported by current evidence.
You might also find helpful:
References
- MRC Vitamin Study Research Group (1991). Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. The Lancet, 338(8760), 131–137. doi:10.1016/0140-6736(91)90133-A
- Greenberg, J.A., Bell, S.J., Guan, Y. & Yu, Y. (2011). Folic Acid Supplementation and Pregnancy: More Than Just Neural Tube Defect Prevention. Reviews in Obstetrics and Gynecology, 4(2), 52–59. PMC3218540
- Gaskins, A.J., Chiu, Y.H., Williams, P.L. et al. (2014). Dietary Folate and Reproductive Success Among Women Undergoing Assisted Reproduction. Obstetrics & Gynecology, 124(4), 801–809. doi:10.1097/AOG.0000000000000477
- Cueto, H.T. & Riis, A.H. (2022). Active Folate Versus Folic Acid: The Role of 5-MTHF (Methylfolate) in Human Health. Integrative Medicine: A Clinician's Journal, 21(3), 36–41. PMC9380836
- US Preventive Services Task Force (2023). Folic Acid Supplementation to Prevent Neural Tube Defects: Updated Evidence Report and Systematic Review. JAMA, 330(5), 454–463. doi:10.1001/jama.2023.9864
- Schisterman, E.F., Sjaarda, L.A., Clemons, T. et al. (2020). Effect of Folic Acid and Zinc Supplementation in Men on Semen Quality and Live Birth. JAMA, 323(1), 35–48. doi:10.1001/jama.2019.18714
- Czeizel, A.E. & Dudás, I. (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. New England Journal of Medicine, 327(26), 1832–1835. doi:10.1056/NEJM199212243272602
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult your doctor, midwife, or a registered healthcare professional before starting or changing any supplement regimen, especially during preconception or pregnancy. Danielle Bowen (MSc, RNutr) is a registered nutritionist — not a doctor. Individual needs vary based on medical history, genetics, and current health status.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











