Best Prenatal Vitamins for Fertility: What to Look for and What to Avoid
A registered fertility nutritionist's guide to choosing the right prenatal vitamin — which nutrients matter most, what to avoid, and when to start.


Here's something that shocked me when I first dug into the research: most prenatal vitamins on the market don't actually contain what they should. Not close. A study by Drazba et al. (2023) in the American Journal of Perinatology analysed the top 48 over-the-counter prenatals in the US and found that not a single one met the American College of Obstetricians and Gynecologists' recommended levels for all five critical nutrients — folic acid, iron, DHA, vitamin D, and calcium. Over a quarter didn't even have enough folic acid.
That finding changed how I talk to my clients about prenatals. Because the question isn't really "which brand is best?" — it's "do you know what you're actually getting, and is it enough?"
I'm a registered nutritionist (RNutr) and I've spent years working with women trying to conceive. I took prenatals myself during my own fertility journey — through low AMH, two chemical pregnancies, and eventually a healthy pregnancy with my son Bowie. I know what the evidence says, what the labels miss, and what actually matters when you're choosing a prenatal vitamin for fertility.
Key Takeaways
- Start your prenatal at least 3 months before trying to conceive — your eggs take ~90 days to mature, and neural tube formation begins before most women know they're pregnant
- Look for methylfolate (5-MTHF) rather than folic acid — up to 40% of women have an MTHFR gene variant that reduces folic acid conversion
- Most prenatals fall short on DHA, choline, and vitamin D — you may need separate supplements to fill the gaps
- Avoid prenatals with retinol (preformed vitamin A) above 3,000IU — high doses are linked to birth defects
- Price doesn't predict quality — a 2023 analysis found no correlation between cost and nutrient adequacy
When to Start Taking Prenatal Vitamins
Most guidance says "start when you're trying to conceive." I tell my clients to start earlier — at least three months before, ideally a year. Here's why that matters so much.
Your eggs aren't created overnight. Each egg takes approximately 90 days to mature from a dormant follicle to a ready-to-ovulate oocyte. The nutritional environment during that maturation window directly influences egg quality — and by extension, your chances of conception and a healthy pregnancy. Adams et al. (2022) reviewed over 200 studies and found that sub-optimal intake of essential nutrients from preconception through pregnancy increases the risk of complications including miscarriage, gestational diabetes, preeclampsia, and neural tube defects.
And here's the timing detail that catches people out: the neural tube — which becomes your baby's brain and spinal cord — forms and closes between days 17 and 30 after conception. That's before most women even take a pregnancy test. If you're not already supplementing with adequate folate by then, you've missed the window where it matters most for preventing spina bifida and other neural tube defects.
The NHS recommends 400 micrograms of folic acid daily from before conception until at least week 12 of pregnancy, plus 10 micrograms of vitamin D throughout pregnancy and while breastfeeding. ACOG in the US recommends similar baseline folate but adds iron, DHA, calcium, and other nutrients to the list. Both agree on one thing: start before you conceive.
The Nutrients That Actually Matter
Not every vitamin and mineral on a prenatal label deserves equal attention. Some are backed by decades of clinical trials. Others are marketing additions that sound good but have limited evidence for fertility or pregnancy. These are the key nutrients I look for — and what the research supports.
Folate (400–800mcg) — This is the non-negotiable. Folate is essential for DNA synthesis, cell division, and neural tube formation. The evidence that folate can help prevent birth defects is so strong that over 80 countries now mandate folic acid fortification in grain products. But there's a nuance worth knowing: up to 40% of the population carries a variant of the MTHFR gene that reduces your body's ability to convert synthetic folic acid into its active form, L-methylfolate. Scaglione & Panzavolta (2014) in Nutrients concluded that supplementation with L-methylfolate should be "strongly considered" given the high prevalence of these polymorphisms. If you don't know your MTHFR status, choosing a prenatal with methylfolate (also listed as 5-MTHF or L-5-methyltetrahydrofolate) covers all bases.
Iron (27mg) — Iron deficiency anaemia affects up to 27.5% of pregnant women in their third trimester (Adams et al., 2022). Your blood volume increases by roughly 45% during pregnancy, and iron is essential for making the extra red blood cells that carry oxygen to your baby. But iron also matters before pregnancy — low iron can disrupt ovulation, and adequate iron intake may help reduce the risk of ovulatory infertility. Look for gentle forms like iron bisglycinate, which cause fewer digestive side effects than ferrous sulphate.
Vitamin D (600–4,000IU) — The NHS recommends just 10mcg (400IU) daily, but emerging evidence suggests this may not be enough. A meta-analysis by Chu et al. (2018) in Human Reproduction found that women with sufficient vitamin D levels were 46% more likely to achieve clinical pregnancy through IVF than those with deficient levels. Vitamin D receptors exist in the uterus, ovaries, and placenta — it's not just a bone vitamin. I took 1,000IU daily during my own preconception period, though your GP can test your levels and advise a specific dose.
DHA (200–300mg) — Docosahexaenoic acid, an omega-3 fatty acid, supports fetal brain and eye development. The problem? Most prenatal tablets don't contain any DHA — it usually comes in a separate softgel. The international expert consensus published by Koletzko et al. (2025) in Nutrients lists DHA as one of 14 essential micronutrients for the preconception and pregnancy periods. If your prenatal doesn't include it, you'll need a standalone omega-3 supplement. Look for at least 200mg DHA specifically (not just total omega-3).
Choline (450mg — good luck finding this in a prenatal) — This is the nutrient the prenatal industry has largely ignored. Choline is essential for neural tube formation, brain development, and liver function. Giannì et al. (2023) called it "a cornerstone of prenatal care" in their review in Nutrients. The adequate intake during pregnancy is 450mg/day, yet most prenatals contain zero choline, or at most 50–55mg. You'll almost certainly need to supplement separately or eat choline-rich foods like eggs (one large egg contains about 147mg), liver, and salmon.
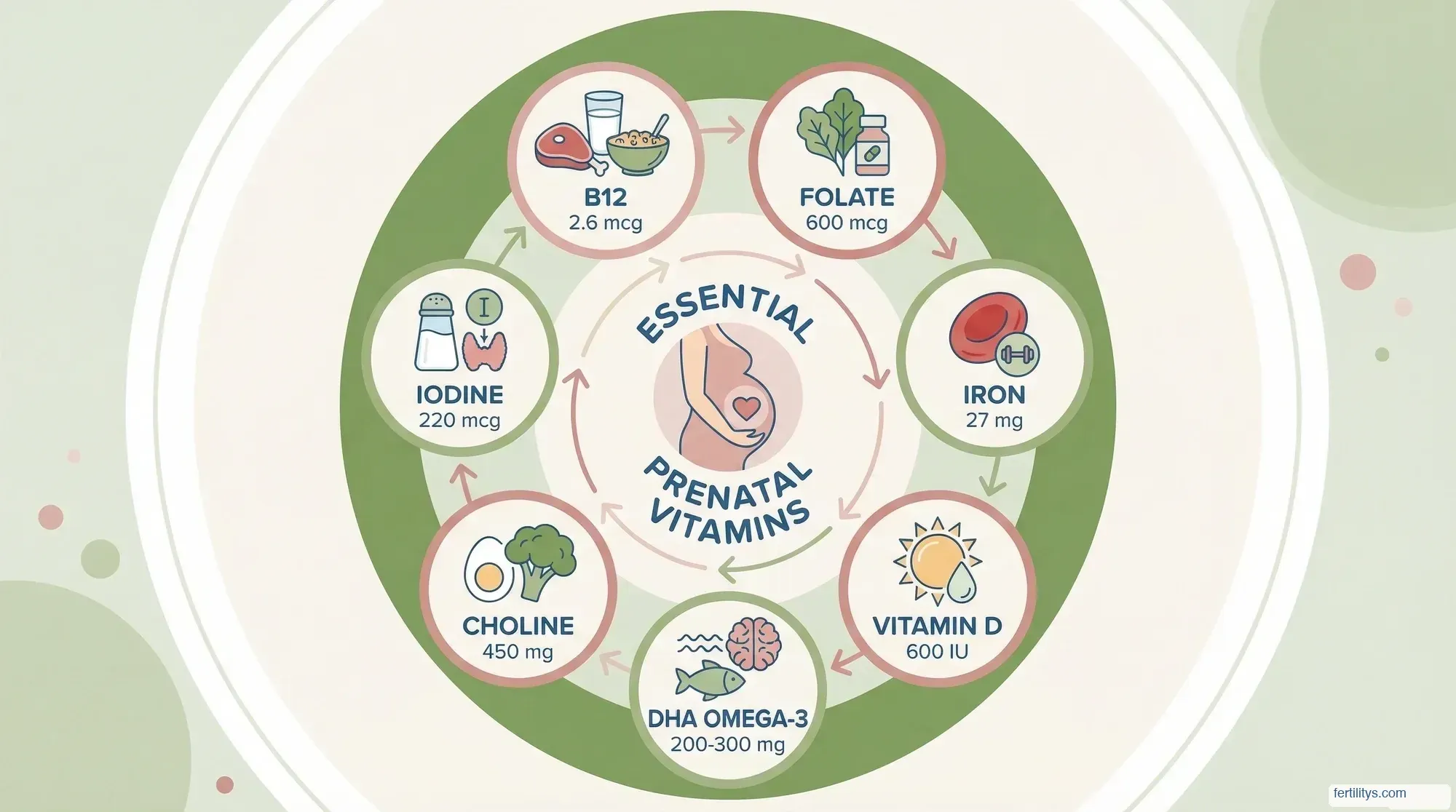
Iodine (150–220mcg) — Iodine supports thyroid function, which directly affects fertility and pregnancy outcomes. Thyroid hormones regulate ovulation, and even mild iodine deficiency during pregnancy is linked to impaired cognitive development in children. The UK doesn't fortify salt with iodine (unlike the US and many other countries), which makes supplementation particularly important for women in Britain — especially if you don't eat much dairy or fish.
Vitamin B12 (2.6mcg) — Works alongside folate in DNA synthesis and red blood cell formation. Deficiency is more common in vegetarian and vegan women, but even meat-eaters can fall short. Low B12 during preconception has been associated with increased miscarriage risk and neural tube defects independently of folate status.
CoQ10 (200–600mg — not in standard prenatals) — Coenzyme Q10 isn't a standard prenatal ingredient, but if you're trying to conceive — especially over 35 or with low ovarian reserve — it's worth adding separately. A systematic review by Xu et al. (2020) in Reproductive BioMedicine Online found that CoQ10 supplementation improved clinical pregnancy rates in women undergoing assisted reproduction. I took 200mg daily during my own fertility journey as part of my energy-and-antioxidant protocol, and it's one of the first supplements I discuss with clients who are preparing to conceive.
What to Avoid in a Prenatal Vitamin
Knowing what shouldn't be in your prenatal is just as important as knowing what should.
Retinol (preformed vitamin A) — High doses above 10,000IU (3,000mcg) are teratogenic, meaning they can cause birth defects. The NHS specifically warns pregnant women to avoid supplements containing retinol. Beta-carotene (provitamin A) is safe because your body only converts what it needs. Check the label: if it says "vitamin A as retinyl palmitate" or "retinyl acetate," that's preformed retinol. If it says "as beta-carotene," you're fine.
Unnecessary fillers and artificial colours — Some gummy prenatals contain added sugars (up to 3–4g per serving), artificial sweeteners, and food dyes. These aren't harmful in small amounts, but they're not what you're paying for either. Gummies also tend to contain fewer nutrients across the board because there's a physical limit to what you can pack into a chewable format — most gummy prenatals have no iron and minimal calcium.
Herbal "fertility blends" — Some prenatals marketed for fertility include herbs like vitex (chasteberry), maca, or ashwagandha. While some of these have preliminary evidence for hormone regulation, they can also interact with fertility treatments and medications. If you're considering herbal additions, discuss them with your GP or fertility specialist first — don't rely on a prenatal to get the dosing right.
UK vs US: Different Guidelines, Same Gaps
If you've been reading prenatal advice online, you've probably noticed the recommendations differ depending on which country the article is aimed at. Here's a quick comparison of what each country officially recommends:
| Nutrient | UK (NHS/NICE) | US (ACOG) | What I Recommend |
|---|---|---|---|
| Folic acid | 400mcg | 400–800mcg | 400–800mcg as methylfolate |
| Iron | No routine supp. | 27mg | 27mg (iron bisglycinate) |
| Vitamin D | 10mcg (400IU) | 15mcg (600IU) | 25–50mcg (1,000–2,000IU) |
| DHA | No specific rec. | 200–300mg | 200–300mg minimum |
| Calcium | No routine supp. | 1,000mg | From diet + supp. if needed |
| Iodine | No specific rec. | 150–220mcg | 150mcg (esp. in UK) |
| Choline | No specific rec. | 450mg | 450mg (diet + supp.) |
The UK takes a more conservative, food-first approach — the NHS only universally recommends folic acid and vitamin D supplements during pregnancy. Everything else is considered achievable through a balanced diet. The reality is that most women in the UK aren't meeting their needs through food alone, particularly for iodine, vitamin D, and choline. If you're in the UK, a comprehensive prenatal fills the gaps that official guidance leaves open.
And if you qualify for the Healthy Start scheme, you can get free vitamins containing folic acid, vitamin C, and vitamin D — but these don't include iron, DHA, iodine, or choline. They're a baseline, not a complete prenatal.
How to Choose the Right Prenatal for You
There is no single "best" prenatal vitamin — because the best one depends on your diet, your health history, and your specific needs. But here's the framework I use with my clients:
Step 1: Check the folate form. Methylfolate is preferable to folic acid. If the label says "folic acid," it'll still work for most women, but methylfolate removes the MTHFR uncertainty entirely.
Step 2: Look for iron. If the prenatal doesn't contain iron (many gummies don't), you'll need a separate iron supplement — especially if your ferritin is below 30mcg/L. Your GP can check this with a simple blood test.
Step 3: Check the DHA. Most tablet-based prenatals don't include DHA. You'll either need a prenatal that comes with a separate DHA softgel, or add a standalone omega-3.
Step 4: Look at what's missing. Compare your prenatal against the dosage table above. Almost no prenatal covers everything adequately — that's normal. The ones I recommend to clients are prenatals that get the core five right (folate, iron, vitamin D, DHA, iodine) and then we fill choline, CoQ10, and extra vitamin D separately if needed.
Step 5: Consider your body. If you have a sensitive stomach, look for iron bisglycinate and consider taking your prenatal with food at night. If you're vegan, make sure your prenatal includes B12 and algae-based DHA (not fish oil). If you're dealing with morning sickness, a smaller capsule or split dose may be easier to keep down.

The Bottom Line
A good prenatal vitamin is one of the simplest, most evidence-backed things you can do when you're trying to conceive. But "good" isn't the same as "expensive" or "popular." It means checking the label, understanding what each nutrient does, and filling the gaps your prenatal leaves behind.
Start early — ideally months before you plan to conceive. Choose methylfolate over folic acid if you can. Make sure iron and DHA are covered, even if that means adding a separate supplement. And don't assume any single product has everything you need, because the research consistently shows that most don't.
Your body is building the environment your future baby will develop in. The nutrients you take now — during this preconception window — shape egg quality, implantation success, and early fetal development in ways that can't be caught up later. That's not pressure. That's empowerment. You can actually do something about it, starting today.
▸Can I just take a regular multivitamin instead of a prenatal?
A standard multivitamin won't have the right balance for pregnancy. Prenatals contain higher levels of folate, iron, and iodine, and lower levels of vitamin A (retinol), which can be harmful in excess during pregnancy. Always choose a product specifically formulated as a prenatal.
▸Are gummy prenatal vitamins as effective as tablets?
Gummy prenatals are easier to take if you struggle with large pills, but they typically contain fewer nutrients — most have no iron and less calcium. If you prefer gummies, plan to supplement iron and possibly other nutrients separately. Check the label rather than assuming all formats are equal.
▸Is it safe to take prenatal vitamins when not pregnant?
Yes — prenatals are safe to take before pregnancy and are specifically recommended during the preconception period. Starting 1–3 months before trying to conceive gives your body time to build adequate nutrient stores. The only caution is the iron content: if you're not planning pregnancy and don't have low iron, a standard women's multivitamin may be more appropriate.
▸What are the best prenatal vitamins in the UK?
In the UK, look for a prenatal that includes methylfolate (not just folic acid), at least 10mcg vitamin D, iron, and iodine — since British diets tend to be low in iodine compared to countries that fortify salt. The free Healthy Start vitamins cover folic acid, vitamin D, and vitamin C, but you'll need additional supplements for iron, DHA, and choline. Brands available in the UK that offer comprehensive formulations include Wild Nutrition, Proceive, and Cytoplan.
▸Should I keep taking prenatal vitamins while breastfeeding?
Yes. The NHS recommends continuing vitamin D supplementation while breastfeeding, and many nutrients — including DHA, iodine, and choline — remain important for your baby's development through breast milk. Most healthcare providers suggest continuing your prenatal throughout breastfeeding, or switching to a postnatal-specific formulation if one is available.
References
- Adams JB, Sorenson JC, Pollard EL, et al. Evidence-based recommendations for an optimal prenatal supplement for women in the US: vitamins and related nutrients. Matern Health Neonatol Perinatol. 2022;8:4. doi:10.1186/s40748-022-00139-9
- Drazba MA, Garner CD, Engstrom JL, et al. Commercially available prenatal vitamins do not meet American College of Obstetricians and Gynecologists nutritional guidelines. Am J Perinatol. 2023;41(Suppl 1):e2547–e2554. doi:10.1055/a-2125-1148
- Scaglione F, Panzavolta G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica. 2014;44(5):480–488. doi:10.3109/00498254.2013.845705
- Chu J, Gallos I, Tobias A, et al. Vitamin D and assisted reproductive treatment outcome: a systematic review and meta-analysis. Hum Reprod. 2018;33(1):65–80. doi:10.1093/humrep/dex326
- Giannì ML, Bezze EN, Colombo L, et al. Choline supplementation in pregnancy: current evidence and implications. Nutrients. 2023;15(21):4526. doi:10.3390/nu15214526
- Xu Y, Nisenblat V, Lu C, et al. Does coenzyme Q10 supplementation improve fertility outcomes in women undergoing assisted reproductive technology procedures? A systematic review and meta-analysis. Reprod BioMed Online. 2020;41(5):845–854. doi:10.1016/j.rbmo.2020.07.020
- Koletzko B, Critch JN, Fidler Mis N, et al. International expert consensus on micronutrient supplement use during the early life course. Nutrients. 2025;17(2):322. doi:10.3390/nu17020322
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Supplement needs vary based on individual health, diet, and medical history. Always consult your GP, midwife, or healthcare provider before starting or changing any supplement regimen, especially during pregnancy or while trying to conceive. Danielle Bowen is a registered nutritionist (RNutr), not a medical doctor.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











