PCOS Symptoms: The Complete Guide to Recognising, Diagnosing, and Managing Polycystic Ovary Syndrome
A fertility nutritionist's comprehensive guide to every PCOS symptom — from the obvious (irregular periods, acne, hair growth) to the invisible (fatigue, mood changes, insulin resistance). Plus diagnosis criteria, the four PCOS types, and evidence-based management.


💡 Quick Answer
PCOS affects 1 in 10 women of reproductive age. The most common symptoms are irregular periods, excess hair growth (hirsutism), acne, weight gain, and thinning hair. But PCOS looks different in everyone — you can be slim, have clear skin, and still have it. Diagnosis requires 2 of 3 criteria: irregular cycles, signs of excess androgens, or polycystic ovaries on ultrasound.
It took me almost two years to get my PCOS diagnosis. Not because the symptoms weren't there — they absolutely were — but because nobody connected the dots. I had irregular periods that my GP put down to stress. Chin hairs I was told were "just hormonal." Fatigue that everyone blamed on my busy schedule. It wasn't until I was trying to conceive and saw a specialist that someone actually said the word PCOS.
My experience isn't unusual. A 2023 UK survey found that over two-thirds of women waited more than a year for their PCOS diagnosis, with 7% waiting over a decade. That's not an access problem — it's an awareness problem. PCOS is the most common hormonal condition in women of reproductive age, yet most people don't know what symptoms to look for, and many GPs still miss it.
This guide covers every symptom of PCOS — the obvious ones and the ones nobody talks about. I've included the diagnostic criteria, the different types of PCOS, and — because I know this is what you really want to know — what you can actually do about it.
What Is PCOS?
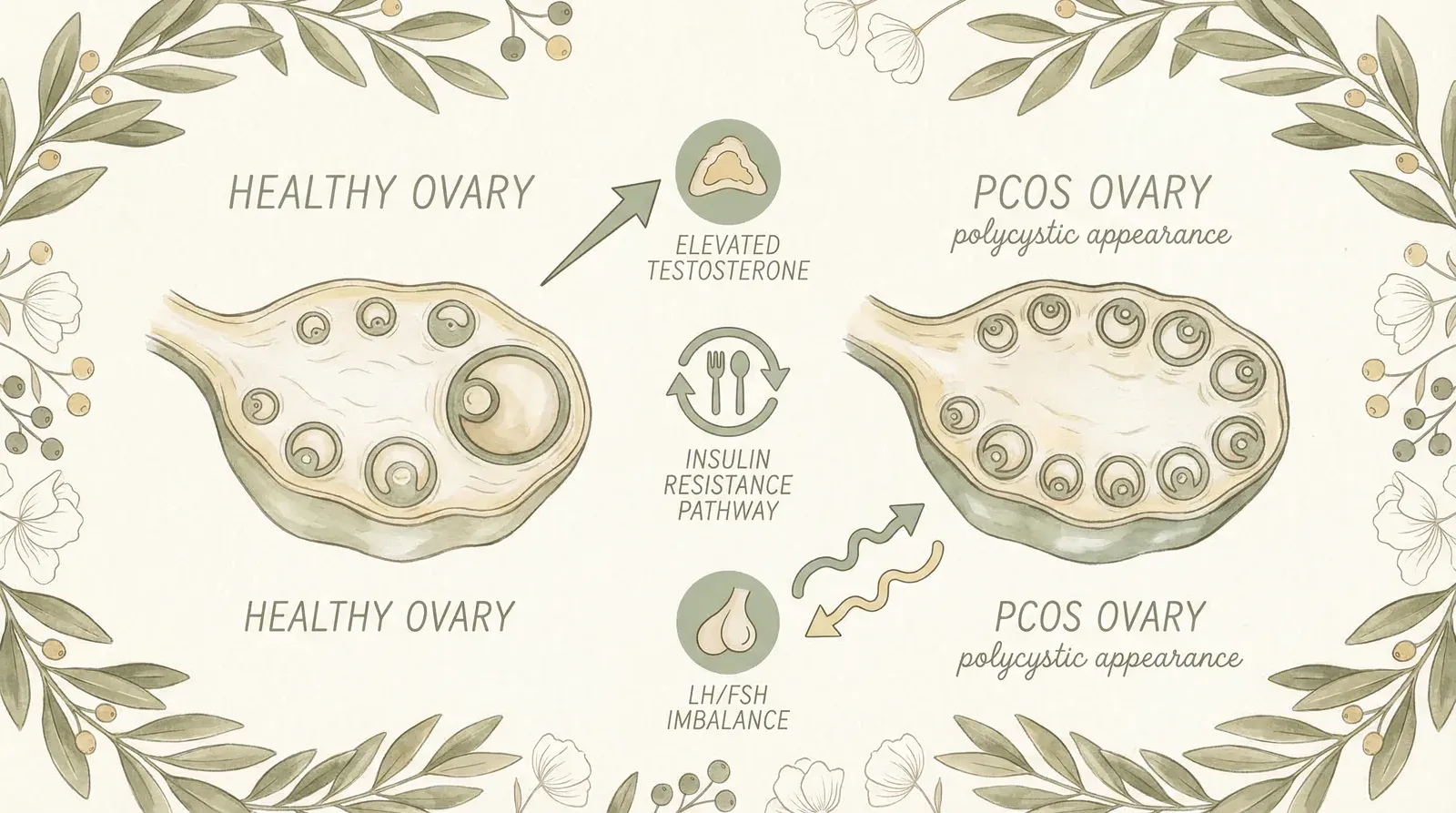
Polycystic ovary syndrome (PCOS) is a hormonal condition that affects how your ovaries work. The name is misleading — you don't actually have "cysts" on your ovaries. What you have are small, undeveloped follicles (egg sacs) that haven't matured properly due to a hormonal imbalance. These show up as a "string of pearls" pattern on an ultrasound, which is where the outdated name comes from.
PCOS involves a combination of:
- Excess androgens — your body produces more testosterone and other "male" hormones than it should. This drives many of the visible symptoms like acne, hair growth, and hair loss.
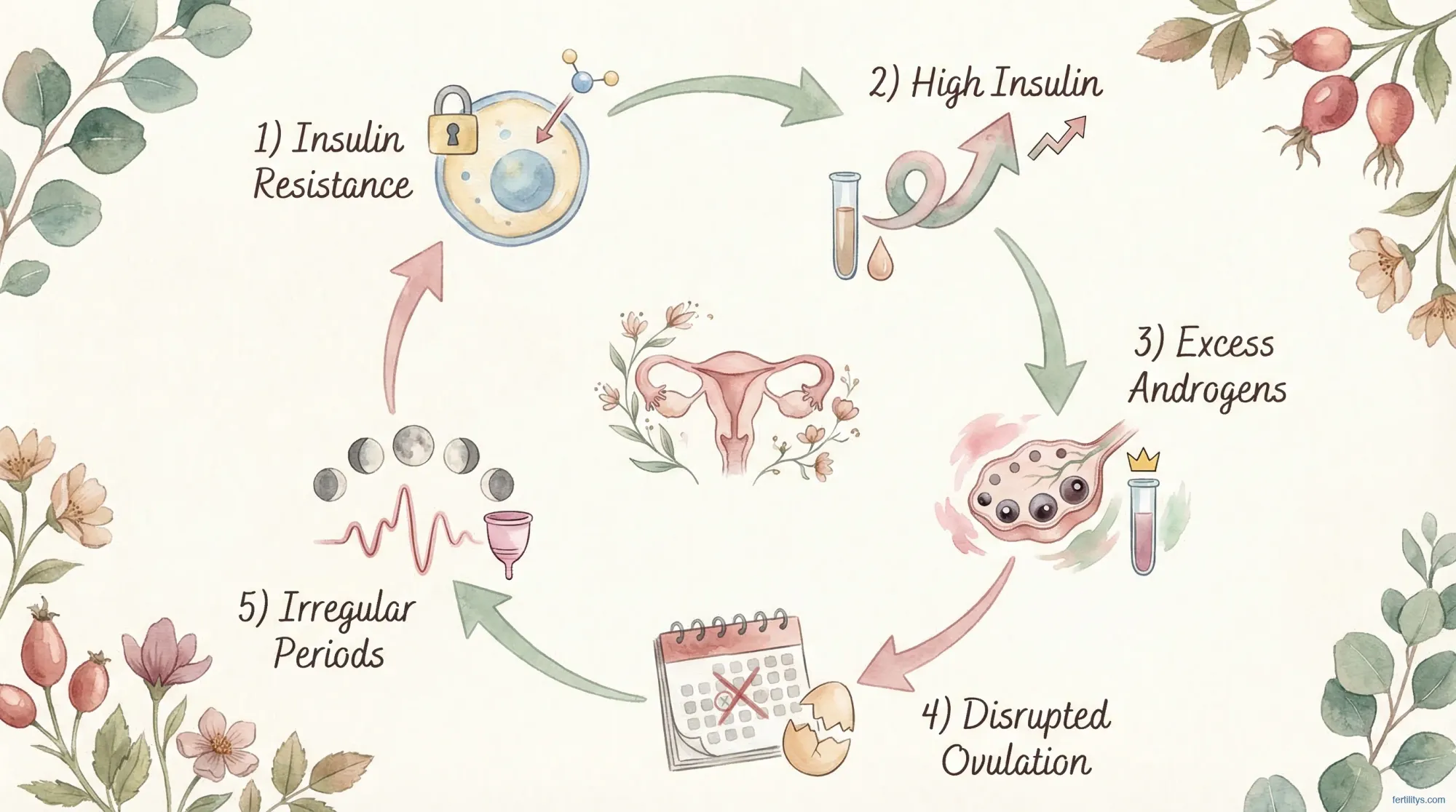
- Insulin resistance — your cells don't respond properly to insulin, so your body produces more of it. High insulin stimulates your ovaries to produce more androgens. It's a vicious cycle.
- Disrupted ovulation — the hormonal imbalance prevents your follicles from maturing and releasing an egg normally, which causes irregular or absent periods.
PCOS affects between 8% and 13% of reproductive-age women worldwide (Bozdag et al., 2016, Human Reproduction Update), making it the most common endocrine disorder in this group. In the UK, that's roughly 1 in 10 women. But because the symptoms vary so much from person to person, up to 70% of women with PCOS remain undiagnosed (March et al., 2010).
The Core Symptoms of PCOS
PCOS doesn't look the same in everyone. That's partly why it's so often missed. But there are core symptoms that most women with PCOS experience to some degree. I'm going to go through each one in detail — what it actually looks and feels like, not just the textbook definition.
1. Irregular Periods
This is the most common symptom, affecting around 75-85% of women with PCOS. "Irregular" can mean:
- Cycles longer than 35 days — you might go 6, 8, or even 12 weeks between periods
- Fewer than 8 periods per year
- Complete absence of periods (amenorrhoea) — some women go months or years without one
- Unpredictable timing — you never know when it's coming. Could be 28 days, could be 50.
- Very heavy periods when they do arrive — because the uterine lining has been building up for longer
The reason: without regular ovulation, your body doesn't produce the normal progesterone surge that triggers a period. Your uterine lining keeps building up until it eventually sheds on its own — often heavily and painfully.
I remember tracking my cycles and having gaps of 6-8 weeks regularly. My GP said "some women just have long cycles" and left it at that. If your cycles are consistently over 35 days, push for investigation. That's not normal variation — it's a symptom worth exploring.
2. Excess Hair Growth (Hirsutism)
Hirsutism — coarse, dark hair growing in places you'd rather it didn't — is the most visible androgen-driven symptom. A 2017 cross-sectional study of 100 women with PCOS found that 78% had hirsutism (Vaidya et al., Indian Journal of Dermatology). It typically affects:
- Face — chin, upper lip, jawline, sideburns
- Chest — around the nipples and between the breasts
- Stomach — a dark line from navel to pubic bone, or more widespread
- Lower back
- Inner thighs
This isn't the fine "peach fuzz" everyone has. This is thick, coarse, pigmented hair — the kind that grows back quickly after shaving and can cause ingrown hairs and scarring. It's driven by excess testosterone converting to dihydrotestosterone (DHT) in the hair follicle.
The emotional impact of hirsutism is massive and consistently underestimated by clinicians. I've had clients who won't leave the house without checking their chin first. Who cancel plans because they're having a bad face-hair day. It's not vanity — it's a genuine quality-of-life issue, and the 2023 international PCOS guidelines now formally recognise its psychological burden (Teede et al., 2023).
3. Acne
PCOS-related acne is different from teenage acne. It tends to be:
- Hormonal in pattern — concentrated along the jawline, chin, and lower cheeks (the "beard area")
- Deep and cystic — painful, under-the-skin bumps rather than surface whiteheads
- Persistent — doesn't respond well to standard acne treatments
- Cyclical — may flare around your period (or where your period would be)
The same 2017 study found acne in 48% of women with PCOS. It's caused by androgens stimulating excess sebum (oil) production in your skin. If you're dealing with persistent jawline acne that doesn't respond to typical skincare, it's worth asking your GP to check your androgen levels.
4. Weight Gain and Difficulty Losing Weight
Between 40-80% of women with PCOS carry excess weight, and the pattern is often distinctive — concentrated around the abdomen rather than the hips and thighs. This is what some people call "PCOS belly," though I'm cautious about that term because it can feel reductive.
The weight issue in PCOS is driven by insulin resistance. When your cells don't respond properly to insulin, your body stores more glucose as fat — particularly visceral fat around your organs and midsection. And here's what makes it so frustrating: the same insulin resistance that causes the weight gain also makes it significantly harder to lose weight through conventional dieting.
I work with a lot of PCOS clients on nutrition, and the first thing I tell them is: if you've been calorie-restricting and exercising intensely and the scale won't budge, it's not your willpower. It's your biology. PCOS requires a different approach — blood sugar management, anti-inflammatory eating, and gentle rather than intense exercise.
5. Hair Thinning and Loss
While excess hair grows where you don't want it, the hair on your head may be thinning — a cruel irony that many women with PCOS find devastating. Androgenic alopecia (female pattern hair loss) affects about 31% of women with PCOS (Vaidya et al., 2017).
The pattern is typically:
- Widening of the centre part
- Overall thinning across the crown — not bald patches, but reduced density
- More hair in the brush, in the shower drain, on your pillow
- Hair that feels finer and more fragile than it used to
This is caused by the same DHT that drives hirsutism — but on the scalp, DHT miniaturises the hair follicles instead of stimulating them. It's another reason to get your androgens checked if you're noticing unexplained hair changes.

The Symptoms Nobody Talks About
PCOS isn't just periods, hair, and acne. There's a whole set of symptoms that rarely make the headline lists but affect daily life profoundly.
Fatigue
Bone-deep, unrelenting tiredness is one of the most reported PCOS symptoms, yet it rarely makes the headline lists. I'd estimate 80% of my PCOS clients mention fatigue as one of their top three complaints — but it's almost never the symptom that led to their diagnosis.
The fatigue in PCOS comes from multiple directions at once:
- Insulin resistance — your cells can't efficiently convert glucose to energy, so you're running on a depleted battery even when you've eaten enough
- Disrupted sleep — sleep apnoea is far more common in PCOS than most people realise (more on this below)
- Chronic inflammation — elevated inflammatory markers like CRP and IL-6 create a constant low-grade immune activation that drains energy
- Vitamin D deficiency — extremely prevalent in PCOS and independently linked to fatigue
- The emotional load — managing visible symptoms, worrying about fertility, dealing with dismissive doctors — it's exhausting
If you're sleeping 8 hours and still waking up feeling like you've been hit by a bus, that's not laziness. That's PCOS. Get your fasting insulin, vitamin D, and iron/ferritin checked — all three are commonly low in PCOS and all three cause fatigue independently.
Mood Changes, Anxiety, and Depression
The 2023 international PCOS guidelines explicitly state that women with PCOS should be screened for anxiety and depression. This isn't incidental — it's integral to the condition. A 2025 review in Frontiers in Global Women's Health confirmed significantly higher rates of both depression and anxiety in women with PCOS compared to controls.
The causes are both biochemical (hormone imbalances affect neurotransmitters) and psychosocial (living with visible symptoms like hirsutism, acne, and weight gain takes a toll on self-esteem and body image).
Skin Darkening (Acanthosis Nigricans)
Dark, velvety patches of skin — typically in the folds of your neck, armpits, groin, and under the breasts. This affects around 30% of women with PCOS and is a direct marker of insulin resistance (Vaidya et al., 2017). It's not a hygiene issue (a misconception that causes real distress) — it's a metabolic signal.
Skin Tags
Small, soft skin growths, often in the same areas as acanthosis nigricans. Found in about 9% of women with PCOS. Like skin darkening, they're linked to insulin resistance and elevated insulin levels.
Headaches
Hormone fluctuations — particularly oestrogen dominance and androgen excess — can trigger frequent headaches or migraines, especially around where your period would normally fall.
Sleep Problems
Women with PCOS are significantly more likely to have sleep apnoea (a condition where breathing repeatedly stops and starts during sleep) and general sleep disruption. This feeds back into the fatigue cycle and worsens insulin resistance — because poor sleep independently raises insulin levels.
Lean PCOS: The Type That Gets Missed
One of the biggest misconceptions about PCOS is that you need to be overweight to have it. You don't. Approximately 20-30% of women with PCOS have a normal BMI — a presentation known as "lean PCOS" (Sachdeva et al., 2019, Journal of Human Reproductive Sciences).
Lean PCOS is consistently underdiagnosed because it doesn't fit the stereotype. If you're slim with irregular periods, a GP is less likely to think "PCOS" and more likely to blame stress, exercise, or undereating. But the research is clear: lean women with PCOS still have significant hormonal disruption, and — critically — they still have insulin resistance, just to a lesser degree than their heavier counterparts.
The symptoms of lean PCOS tend to be:
- Irregular or absent periods (still the primary marker)
- Acne (often more prominent than hirsutism in lean PCOS)
- Mild hirsutism
- Difficulty conceiving despite appearing healthy
- Elevated androgens on blood tests, even with a normal BMI
- Polycystic ovaries on ultrasound
If you're at a healthy weight but struggling with irregular cycles and acne, don't let anyone tell you it can't be PCOS. Push for the blood tests. I've seen too many lean PCOS clients who were dismissed for years before someone finally ran the right panel.
PCOS and Fertility: What You Need to Know
PCOS is the leading cause of anovulatory infertility — meaning infertility caused by not ovulating regularly. But — and I really want to emphasise this — having PCOS does not mean you can't get pregnant. It means getting pregnant may take more planning, support, and patience.
The fertility picture with PCOS is more nuanced than most people are told:
- Many women with PCOS do ovulate — just irregularly. If you're having periods (even irregular ones), you're likely ovulating at least some of the time.
- AMH is typically elevated in PCOS — which means you actually have more follicles than average. The issue isn't egg quantity — it's getting those follicles to mature and release properly.
- Lifestyle changes can restore ovulation — research consistently shows that even a 5-10% reduction in body weight can restart regular cycles in women with PCOS who carry excess weight (Kiddy et al., 1992; Clark et al., 1998).
- Myo-inositol supplementation improves ovulation rates and insulin sensitivity in PCOS — I've written about this in detail in my myo-inositol and PCOS guide.
- Medical options exist — letrozole (now first-line over clomiphene per the 2023 guidelines), metformin for insulin resistance, and IVF for more complex cases.
I work with a lot of PCOS clients on preconception nutrition, and I always give them the same starting point: manage your blood sugar, reduce inflammation, and give yourself at least a year of preparation. Not three months — a year. The egg development timeline is 90 days, and the nutritional and lifestyle changes that support ovulation need time to take effect.
How PCOS Is Diagnosed
The current diagnostic standard is the Rotterdam criteria, updated and reinforced by the 2023 International Evidence-based PCOS Guideline (Teede et al., 2023). You need 2 out of 3 of the following:
| Criterion | What It Means | How It's Tested |
|---|---|---|
| 1. Irregular cycles | Fewer than 8 periods per year, or cycles >35 days | Menstrual history |
| 2. Excess androgens | Clinical signs (acne, hirsutism, hair loss) OR elevated androgens on blood test | Physical exam + blood test (free testosterone, DHEA-S, androstenedione) |
| 3. Polycystic ovaries | ≥12 follicles per ovary (2-9mm) or ovarian volume >10ml | Transvaginal ultrasound |
A few important nuances:
- You don't need all three. Two out of three is sufficient for diagnosis.
- You don't need polycystic ovaries to have PCOS. If you have irregular cycles + clinical hyperandrogenism, that's PCOS — even with normal-looking ovaries on ultrasound.
- The 2023 guidelines now allow AMH as an alternative to ultrasound for confirming polycystic ovaries in adults. An elevated AMH (typically >3.8-5.0 ng/mL depending on assay) can substitute for the ultrasound criterion.
- Other conditions must be ruled out first — thyroid disorders, congenital adrenal hyperplasia, Cushing's syndrome, and hyperprolactinaemia can all mimic PCOS symptoms.
Blood Tests Your GP Should Order
If you suspect PCOS, ask your GP for the following panel:
- Free testosterone — the most sensitive marker for hyperandrogenism
- Total testosterone
- Sex hormone-binding globulin (SHBG) — low SHBG means more free testosterone
- DHEA-S — to rule out adrenal causes of excess androgens
- LH and FSH — a raised LH:FSH ratio (>2:1) is suggestive of PCOS, though not diagnostic
- AMH — elevated in PCOS; now accepted as alternative to ultrasound
- Thyroid function (TSH) — to rule out thyroid disorders
- Prolactin — to rule out hyperprolactinaemia
- 17-hydroxyprogesterone — to rule out congenital adrenal hyperplasia
- Fasting glucose and insulin — to assess insulin resistance
- HbA1c — long-term blood sugar marker
- Lipid profile — cardiovascular risk assessment
If your GP dismisses your symptoms or only orders TSH, push for the full panel. You're entitled to thorough investigation, especially if you have 2+ symptoms from this article. Print the blood test list above and take it to your appointment if it helps.
The Four Types of PCOS
PCOS isn't one condition with one cause. Current thinking recognises four main phenotypes — and knowing which type you have matters because it changes the treatment approach.
| Type | What's Present | Key Features |
|---|---|---|
| Type A (Classic) | Irregular cycles + high androgens + polycystic ovaries | Most severe. All three criteria present. Highest metabolic risk. |
| Type B (Classic) | Irregular cycles + high androgens | No polycystic ovaries on ultrasound, but still fully diagnosable. |
| Type C (Ovulatory) | High androgens + polycystic ovaries | Regular periods. Often missed because cycles seem "normal." Acne and hirsutism are the giveaway. |
| Type D (Non-hyperandrogenic) | Irregular cycles + polycystic ovaries | No visible androgen symptoms. The "invisible" PCOS — hardest to diagnose. |
Type C is particularly worth knowing about. These are women who have regular periods and think they can't have PCOS — but they do. If you have persistent acne and excess hair growth with regular cycles, a Type C PCOS diagnosis could explain why.
What Causes PCOS?
The honest answer is: we don't fully know. PCOS has a strong genetic component — you're more likely to develop it if your mother or sister has it. But genes aren't destiny. The current understanding is that PCOS develops from a combination of:
- Genetic predisposition — multiple genes involved, each with a small effect (Azziz et al., 2016)
- Insulin resistance — both a cause and a consequence. High insulin stimulates the ovaries to produce more androgens. More androgens worsen insulin resistance. It's a feedback loop.
- Low-grade chronic inflammation — women with PCOS have elevated inflammatory markers (CRP, IL-6) even when controlling for weight. This inflammation contributes to insulin resistance and androgen production.
- Gut microbiome disruption — emerging research suggests the gut plays a role in androgen metabolism and insulin sensitivity. Women with PCOS tend to have less diverse gut bacteria (Lindheim et al., 2017).
- Environmental factors — exposure to endocrine disruptors (BPA, phthalates), stress, diet quality, and exercise patterns all influence whether PCOS manifests and how severely.
This is why I take a whole-body approach with my clients rather than just treating individual symptoms. PCOS isn't a broken ovary — it's a systemic condition with metabolic, hormonal, and inflammatory components that all interact.
Long-Term Health Risks of PCOS
PCOS isn't just a reproductive condition — it's a metabolic one. The same insulin resistance and chronic inflammation that drive your symptoms also increase your long-term health risks. I tell my clients: managing PCOS isn't just about periods and fertility. It's about protecting your health for decades to come.
Type 2 Diabetes
Women with PCOS are 4 to 8 times more likely to develop Type 2 diabetes than women without PCOS (Moran et al., 2010, Human Reproduction Update). The insulin resistance that characterises PCOS progressively worsens if left unmanaged — your pancreas eventually can't keep up with the demand for more and more insulin. Up to 40% of women with PCOS develop prediabetes or Type 2 diabetes by age 40. This is why fasting glucose, fasting insulin, and HbA1c should be checked annually if you have PCOS — not just at diagnosis.
Cardiovascular Disease
PCOS significantly increases your risk of cardiovascular disease through multiple pathways: dyslipidaemia (elevated LDL, low HDL, high triglycerides), hypertension, chronic inflammation, and endothelial dysfunction. A 2020 meta-analysis found women with PCOS had a 2-fold increased risk of coronary heart disease and stroke compared to controls (de Groot et al., Human Reproduction Update). The 2023 international guidelines now recommend regular cardiovascular risk assessment — including lipid profiles — for all women with PCOS.
Endometrial Hyperplasia and Cancer
When you don't ovulate regularly, your uterine lining (endometrium) doesn't shed monthly as it should. Instead, it keeps thickening under the influence of unopposed oestrogen — without the progesterone that would normally cause it to shed. Over time, this can lead to endometrial hyperplasia (thickened lining), which in some cases progresses to endometrial cancer. Women with PCOS have a 2.7-fold increased risk of endometrial cancer (Barry et al., 2014, Human Reproduction). This is one reason why long gaps without a period shouldn't be ignored — if you're going more than 3 months without bleeding, speak to your GP about inducing a withdrawal bleed with progesterone.
Sleep Apnoea
Obstructive sleep apnoea (where your breathing repeatedly stops and starts during sleep) is 5 to 30 times more common in women with PCOS than in the general female population. It's driven by the combination of insulin resistance, higher visceral fat, and androgen excess. The symptoms — snoring, waking unrefreshed, daytime fatigue, morning headaches — overlap with general PCOS fatigue, so it's often missed. If you're exhausted despite adequate sleep, ask about a sleep study.
Mental Health
This deserves more than a footnote. A 2020 meta-analysis of 57 studies found women with PCOS were 3 times more likely to have clinical depression and 5 times more likely to have clinical anxiety compared to controls (Cooney et al., Human Reproduction). The causes are both biological (hormonal disruption affects neurotransmitter function, insulin resistance impairs brain glucose metabolism) and psychosocial (the daily burden of visible symptoms, fertility anxiety, diagnostic delays, and feeling dismissed by clinicians). The 2023 guidelines now mandate routine mental health screening for all PCOS patients.
I've had clients break down in tears during our first consultation — not because of the diagnosis itself, but because someone finally took their symptoms seriously. If you're struggling emotionally with PCOS, please know that it's a recognised feature of the condition, not a personal failing. And seek support — whether that's your GP, a therapist familiar with chronic conditions, or a PCOS support community.
PCOS Symptoms by Age
PCOS doesn't present the same way at every stage of life. Knowing what to look for at your age can help you catch it earlier — or understand why your symptoms are changing.
Teens and Early 20s
The most common first symptom is irregular periods after the first year or two of menstruation (some irregularity is normal in the first 1-2 years). Severe acne that doesn't respond to typical treatments is the second most common early sign. Weight gain during this period is often attributed to "hormones" or "growing up" when it could be early PCOS insulin resistance.
Diagnosis in teenagers is tricky because irregular periods and acne are common in adolescence regardless of PCOS. The 2023 guidelines recommend using adult criteria but being cautious — ultrasound-based polycystic ovary criteria shouldn't be used in adolescents because multi-follicular ovaries are normal during puberty.
Mid-20s to 30s
This is when most diagnoses happen — often prompted by fertility difficulties. Symptoms that were dismissed in the teens (irregular periods, persistent acne) are now taken more seriously. Hirsutism typically becomes more noticeable. Weight gain around the midsection may accelerate. Hair thinning may begin.
Late 30s and 40s
Paradoxically, some PCOS symptoms improve with age as androgen levels naturally decline — cycles may become more regular, and acne may improve. But metabolic risks increase: the insulin resistance and inflammation that characterised your PCOS in your 20s and 30s now elevate your risk for Type 2 diabetes, cardiovascular disease, and endometrial thickening. This is why long-term monitoring matters even if your visible symptoms improve.
Managing PCOS Symptoms Naturally
I'm going to focus on what I know best — the nutrition and lifestyle interventions that have the strongest evidence for PCOS management. These aren't alternatives to medical treatment — they work alongside it.
Blood Sugar Management
This is the single most impactful dietary change for PCOS. Because insulin resistance drives so many of the symptoms, stabilising your blood sugar can improve androgens, ovulation, weight, energy, and mood — all at once.
- Pair carbohydrates with protein, fat, or fibre at every meal (never eat carbs alone)
- Choose complex carbs (whole grains, sweet potato, legumes) over refined
- Eat at regular intervals — no long gaps that trigger cortisol and insulin spikes
- Include cinnamon, apple cider vinegar, and chromium-rich foods — all shown to support insulin sensitivity
Anti-Inflammatory Eating

The Mediterranean diet is the most studied dietary pattern for PCOS. A 2022 systematic review found it significantly improved insulin resistance, androgen levels, and menstrual regularity in women with PCOS (Barrea et al., Nutrients). My practical version:
- Oily fish 2-3 times per week (salmon, sardines, mackerel)
- Extra virgin olive oil as your primary cooking fat
- Abundant vegetables — at least 7 portions daily
- Nuts, seeds, and legumes regularly
- Reduce — ideally eliminate — ultra-processed foods, refined sugar, and seed oils
🍎 Go Organic With the Dirty Dozen
These twelve fruits and vegetables carry the heaviest pesticide loads. I tell all my clients: if you can only afford to go organic on some things, make it these. The rest you can buy conventional and wash well.
The list: Strawberries, spinach, kale/collard/mustard greens, peaches, pears, nectarines, apples, grapes, bell & hot peppers, cherries, blueberries, green beans (EWG, 2025).
Key Supplements
- Myo-inositol (4g/day) — the strongest evidence base of any PCOS supplement. Improves insulin sensitivity, androgen levels, and ovulation. I've written a full guide to myo-inositol for PCOS.
- Vitamin D — deficiency is extremely common in PCOS and worsens insulin resistance. Get tested, supplement to sufficiency.
- Omega-3 (EPA/DHA) — reduces inflammation markers and improves lipid profiles in PCOS.
- Magnesium — supports insulin sensitivity, sleep, and stress management. Many PCOS clients are deficient.
- Chromium — enhances insulin receptor function. Modest but consistent evidence in PCOS.

Exercise
This is one area where PCOS advice goes against the grain. Intense exercise (HIIT, CrossFit, heavy running) can actually worsen PCOS symptoms by spiking cortisol — which drives insulin resistance and androgen production. I've seen this pattern repeatedly in my clients.
What works better:
- Strength training 2-3x/week — builds muscle, which improves insulin sensitivity
- Walking daily — 30 minutes after meals helps regulate blood sugar
- Yoga or Pilates — lowers cortisol, supports hormonal balance
- Gentle cardio — swimming, cycling at moderate intensity
Medical Treatments for PCOS
I focus on nutrition and lifestyle because that's my area of expertise — and because the evidence consistently shows they should be first-line for PCOS management. But I'd be doing you a disservice if I didn't cover the medical options, because many women need both lifestyle changes and medication.
Metformin
Originally a diabetes drug, metformin improves insulin sensitivity and can help reduce androgen levels, restore ovulation, and support weight management. The 2023 guidelines recommend it as an adjunct to lifestyle changes for women with PCOS who have insulin resistance or BMI ≥25. I've seen it work brilliantly alongside dietary changes — the combination is often more effective than either alone.
Letrozole (for Fertility)
If you're trying to conceive, letrozole is now the recommended first-line ovulation induction drug — replacing clomiphene citrate, which held that position for decades. It works by temporarily lowering oestrogen, which triggers your pituitary to release more FSH and stimulate follicle development. Success rates are higher than clomiphene with fewer side effects.
Combined Oral Contraceptive Pill
For women not trying to conceive, the pill can regulate cycles, reduce androgen levels, clear acne, and slow hirsutism. It also protects against endometrial hyperplasia by providing regular progesterone exposure. It doesn't treat the underlying insulin resistance, though — which is why I always recommend lifestyle changes alongside it.
Spironolactone (for Androgen Symptoms)
An anti-androgen medication that can significantly reduce hirsutism, acne, and hair loss by blocking testosterone at the receptor level. It takes 6-12 months to see full results and must NOT be used during pregnancy (it can feminise a male foetus). Usually prescribed alongside the pill for this reason.
Myo-Inositol
Technically a supplement rather than a medication, but the evidence base is now strong enough that many endocrinologists prescribe it. 4g daily of myo-inositol improves insulin sensitivity, reduces androgens, and restores ovulation in many women with PCOS. I cover this in depth in my myo-inositol and PCOS guide.
Important: all medication decisions should be made with your doctor, based on your specific PCOS phenotype, symptoms, and goals. What works for Type A PCOS may not be right for Type D.
When to See a Doctor
See your GP if you have any combination of:
- Cycles consistently longer than 35 days or fewer than 8 periods per year
- Persistent acne along the jawline that doesn't respond to standard treatment
- New or worsening hair growth on your face, chest, or stomach
- Hair thinning on your scalp with no obvious cause
- Difficulty getting pregnant after 6+ months of trying
- Unexplained weight gain concentrated around your midsection
- Dark, velvety skin patches in your armpits, neck, or groin
Don't wait for all of these to be present — two symptoms are enough to warrant investigation. And if your GP dismisses you, you have every right to request a referral to a gynaecologist or endocrinologist. The diagnostic blood tests listed earlier in this article are standard — there's no reason not to run them.
The NHS estimates that PCOS affects around 1 in 10 women in the UK, making it one of the most common hormonal conditions in women of reproductive age. While the exact cause of PCOS isn't fully understood, insulin resistance and genetics both play significant roles. Women with PCOS also have an increased risk of developing type 2 diabetes and high blood pressure later in life, which is why early diagnosis and lifestyle management matter so much.
The Bottom Line
PCOS is the most common hormonal condition in women of reproductive age, affecting 1 in 10. But despite being so common, it's still poorly understood, frequently missed, and often dismissed. The average diagnosis takes over a year — and for some women, over a decade.
The symptoms range from the obvious (irregular periods, hirsutism, acne) to the invisible (fatigue, mood changes, insulin resistance). You can have PCOS at any weight, with any combination of symptoms, and with or without polycystic ovaries on ultrasound. If something feels wrong — trust that instinct and push for answers.
And if you've just been diagnosed: take a breath. PCOS is manageable. With the right nutrition, lifestyle changes, and medical support, most women with PCOS can manage their symptoms effectively and conceive when they're ready. It's not a sentence — it's a starting point for taking charge of your health.

🌿 Dani recommends:
If you're managing PCOS, start your morning with this blood-sugar-balancing breakfast bowl I make for my clients: cook 40g oats with water, then stir in 1 tablespoon almond butter, a handful of blueberries, a sprinkle of cinnamon, and 1 tablespoon ground flaxseed. The protein from the almond butter, fibre from the oats and flax, and cinnamon for insulin sensitivity make this one of the best breakfasts for PCOS. I eat a version of this most mornings myself — it keeps me full until lunch without any blood sugar crash.
📖 Get all my recipes & resources →
▸What are the first signs of PCOS?
The most common first signs are irregular periods (cycles longer than 35 days or fewer than 8 per year), persistent hormonal acne along the jawline, and unwanted hair growth on the face, chest, or stomach. In teenagers, severe acne that doesn't respond to standard treatments and irregular periods beyond the first 1-2 years of menstruation are key early warning signs.
▸Can you have PCOS and still have regular periods?
Yes — this is called Type C (ovulatory) PCOS. You can have regular periods but still have excess androgens and polycystic ovaries on ultrasound. If you have persistent acne, hirsutism, or hair thinning with regular cycles, it's worth getting your androgen levels tested. Regular periods don't rule out PCOS.
▸What does PCOS look like on the skin?
PCOS skin symptoms include hormonal acne (deep, cystic, concentrated along the jawline), excess facial and body hair (hirsutism, affecting 78% of women with PCOS), thinning hair on the scalp, dark velvety patches in skin folds called acanthosis nigricans (30% of cases), and small skin tags. These are all driven by excess androgens and insulin resistance.
▸Can you have PCOS at a normal weight?
Yes. Approximately 20-30% of women with PCOS have a normal BMI — this is called "lean PCOS." Lean PCOS is consistently underdiagnosed because it doesn't fit the stereotype. These women still have hormonal disruption and often insulin resistance, just to a lesser degree. If you're slim with irregular periods and acne, don't rule out PCOS.
▸Is PCOS curable?
PCOS can't be cured, but it can be effectively managed. Lifestyle changes (diet, exercise, stress management), supplements (myo-inositol, vitamin D), and medical treatments (metformin, letrozole, anti-androgens) can significantly reduce symptoms and improve quality of life. Many women with well-managed PCOS live with minimal symptoms.
▸Can you get pregnant with PCOS?
Yes. PCOS is the leading cause of anovulatory infertility, but most women with PCOS can conceive with the right support. Lifestyle changes, supplements like myo-inositol, and medications like letrozole can restore ovulation. Even without treatment, many women with PCOS ovulate irregularly — it just may take longer to conceive. Having PCOS does not mean you can't get pregnant.
▸What is the best diet for PCOS?
The Mediterranean diet has the strongest evidence for PCOS management. Focus on blood sugar stabilisation (pair carbs with protein/fat), anti-inflammatory foods (oily fish, olive oil, abundant vegetables), and reducing ultra-processed foods and refined sugar. Specific evidence-based additions include cinnamon for insulin sensitivity and ground flaxseed for androgen reduction.
▸What are the first signs of PCOS?
The most common first signs are irregular periods (cycles longer than 35 days or fewer than 8 per year), persistent hormonal acne along the jawline, and unwanted hair growth on the face, chest, or stomach.
▸Can you have PCOS and still have regular periods?
Yes — this is called Type C (ovulatory) PCOS. You can have regular periods but still have excess androgens and polycystic ovaries on ultrasound.
▸What does PCOS look like on the skin?
Hormonal acne (deep, cystic, along the jawline), excess facial and body hair (78% of cases), thinning scalp hair, dark velvety patches called acanthosis nigricans (30%), and skin tags.
▸Can you have PCOS at a normal weight?
Yes. 20-30% of women with PCOS have normal BMI — called lean PCOS. Often underdiagnosed because it doesn't fit the stereotype.
▸Is PCOS curable?
Not curable, but effectively manageable with diet, lifestyle, supplements (myo-inositol, vitamin D), and medical treatment. Many women live with minimal symptoms.
▸Can you get pregnant with PCOS?
Yes. Most women with PCOS can conceive with lifestyle changes, supplements like myo-inositol, and/or medications like letrozole.
▸What is the best diet for PCOS?
Mediterranean diet with blood sugar stabilisation. Pair carbs with protein/fat, eat anti-inflammatory foods (oily fish, olive oil, vegetables), reduce processed foods.
▸What are the first signs of PCOS?
Common early signs include irregular or absent periods, acne (especially jawline), excess facial or body hair, weight gain around the middle, thinning scalp hair, and difficulty getting pregnant. Not all women experience all symptoms.
▸Can you have PCOS with regular periods?
Yes. About 20-30% of women with PCOS have regular cycles. PCOS diagnosis requires 2 of 3 criteria: irregular periods, elevated androgens (blood test or symptoms), and polycystic ovaries on ultrasound. You don't need all three.
▸At what age does PCOS usually start?
PCOS symptoms often become noticeable during late teens or early twenties, though it can develop at any reproductive age. Many women aren't diagnosed until their late 20s or 30s when they start trying to conceive and discover irregular ovulation.
You might also find helpful:
References
- Teede HJ et al. (2023). Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Journal of Clinical Endocrinology & Metabolism, 108(10):2447-2469. doi:10.1210/clinem/dgad463
- Bozdag G et al. (2016). The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Human Reproduction, 31(12):2841-2855. doi:10.1093/humrep/dew218
- March WA et al. (2010). The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Human Reproduction, 25(2):544-551. doi:10.1093/humrep/dep399
- Vaidya R et al. (2017). Cutaneous Manifestations of Polycystic Ovary Syndrome: A Cross-Sectional Clinical Study. Indian Journal of Dermatology, 62(2):168-171. doi:10.4103/ijd.IJD_304_16
- Sachdeva G et al. (2019). Comparison of the Different PCOS Phenotypes Based on Clinical Metabolic, and Hormonal Profile, and their Response to Clomiphene. Indian Journal of Endocrinology and Metabolism, 23(3):326-331.
- Lindheim L et al. (2017). Alterations in Gut Microbiome Composition and Barrier Function Are Associated with Reproductive and Metabolic Defects in Women with Polycystic Ovary Syndrome. PLoS One, 12(1):e0168390. doi:10.1371/journal.pone.0168390
- Barrea L et al. (2022). Mediterranean Diet and PCOS: A Systematic Review. Nutrients, 14(12):2538. doi:10.3390/nu14122538
- Azziz R et al. (2016). Polycystic ovary syndrome. Nature Reviews Disease Primers, 2:16057. doi:10.1038/nrdp.2016.57
- Kiddy DS et al. (1992). Improvement in endocrine and ovarian function during dietary treatment of obese women with polycystic ovary syndrome. Clinical Endocrinology, 36(1):105-111.
- Fertility Family (2023). PCOS Awareness Survey 2023. Full report
Medical Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider about your symptoms. PCOS diagnosis requires clinical assessment — an online article cannot diagnose you. Danielle Bowen is a registered nutritionist (RNutr), not a medical doctor.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











