Male Fertility: How to Improve Sperm Quality Naturally
Half of all fertility issues involve sperm — yet most couples focus only on the woman. A fertility nutritionist explains what the science says about supplements, diet, lifestyle, and the 74-day rule.


Quick answer: Around half of all fertility difficulties involve a male factor, yet sperm health is often the last thing couples investigate. The good news? Sperm regenerate every 74 days, which means targeted changes to diet, supplements, and lifestyle can produce measurable improvements within three months. The strongest evidence supports CoQ10, zinc, selenium, and omega-3 fatty acids — alongside cutting heat exposure, quitting smoking, and reducing alcohol.
Key takeaways
- Male factor infertility contributes to roughly 50% of cases — it's not just a "her" problem
- A semen analysis (SA) is the starting point, but one bad result isn't a diagnosis
- Sperm take approximately 74 days to develop, so give any intervention at least three months
- Antioxidant supplements (especially CoQ10 at 200–400 mg/day) have the strongest clinical evidence for improving sperm parameters
- Lifestyle factors — heat, smoking, alcohol, weight, sleep — have a direct and often reversible impact on sperm quality
When we started trying to conceive, I'll be honest — most of my energy went into tracking my own cycles, monitoring my AMH levels, and building my nutrition protocol. It took me longer than it should have to realise that fertility isn't a solo project. And I know I'm not the only one.
The conversation around fertility is still overwhelmingly focused on women. We do the tracking, we take the supplements, we sit in the clinic waiting rooms. But the research is unambiguous: male factor infertility is involved in around 50% of couples struggling to conceive (Kumar & Singh, 2015). That's not a footnote — it's half the story.
What frustrates me most is how often men are left out of the conversation entirely. I've worked with women who've spent months — sometimes years — investigating their own health before anyone suggested their partner get a basic semen analysis. And when results do come back less than ideal, the panic is immediate. I get it. But here's what I want you to take away from this article: sperm quality is remarkably responsive to change. Unlike egg reserve, which declines with age and can't be replenished, sperm are produced fresh every 74 days. That's a window of opportunity most couples don't realise they have.
What a Semen Analysis Actually Tells You
A semen analysis is the single most important diagnostic tool for male fertility. It's straightforward, non-invasive, and can be done through your GP or a fertility clinic. But the results can look intimidating — so let's break down what matters.
The key parameters
The World Health Organisation updated its reference values in 2021 (WHO, 2021), and these are the benchmarks your doctor will use:
| Parameter | WHO 6th Edition Reference (5th centile) |
|---|---|
| Semen volume | ≥1.4 mL |
| Sperm concentration | ≥16 million/mL |
| Total sperm count | ≥39 million per ejaculate |
| Total motility | ≥42% |
| Progressive motility | ≥30% |
| Normal morphology (strict criteria) | ≥4% |
One thing that catches people off guard: these are 5th centile values, not averages. Being at or just below these numbers doesn't necessarily mean something is wrong — it means you're in the lower range of men who went on to conceive within 12 months. Context matters enormously here.
One bad result isn't a diagnosis
NICE guidelines are clear on this: if the first semen analysis comes back abnormal, a repeat test should be done three months later to account for the full spermatogenesis cycle (NICE, 2025). Sperm quality fluctuates — illness, stress, a recent fever, even the time of year can shift results. I've seen couples spiral after a single suboptimal SA, and that anxiety itself can make things worse.
The exception? If results show severe oligozoospermia (very low count) or azoospermia (no sperm at all), the repeat test should happen sooner rather than later.
Sperm Morphology: Why 1% Isn't the Disaster You Think
If there's one number that causes more unnecessary panic than any other in male fertility, it's morphology. I see it constantly — a result comes back showing 1% or 2% normal forms under Kruger strict criteria, and couples assume the worst.
Here's what the research actually shows: morphology is the least predictive of the three main parameters (count, motility, and morphology) when it comes to natural conception. The strict criteria used in modern labs mean that even perfectly fertile men routinely score in the low single digits. A 2012 study published in Human Reproduction found that morphology below 4% had minimal impact on time to pregnancy when count and motility were normal (Hotaling et al., 2012).
That doesn't mean morphology is irrelevant — in IVF/ICSI cycles, it does matter more. But if your partner's SA shows low morphology alongside decent count and motility, that alone is not a reason to panic. What it is, though, is a prompt to look at the bigger picture: oxidative stress, diet, toxin exposure, and lifestyle factors that can affect how sperm develop.
Beyond the Numbers: Why Sperm Quality Runs Deeper Than Count
A standard semen analysis tells you three things: how many sperm there are, how well they move, and what they look like. What it doesn't tell you is whether the DNA inside those sperm is intact.
DNA fragmentation — the hidden factor
Sperm DNA fragmentation (SDF) testing measures how much damage exists in the genetic material sperm carry. A standard SA can come back completely normal while DNA fragmentation is critically high. This matters because elevated SDF is linked to reduced fertilisation rates, failed IVF cycles, and recurrent miscarriage (Agarwal et al., 2020).
SDF testing isn't routine in the UK — your GP won't offer it unless you ask, and even then, you may need to go private. But if you've experienced unexplained infertility, recurrent pregnancy loss, or repeated IVF failure with good-looking embryos, it's worth requesting. A 2024 meta-analysis in Scientific Reports found that antioxidant supplementation and varicocelectomy were the most effective interventions for reducing SDF (Assessing the efficacy of varicocelectomy, antioxidants, FSH treatment, and lifestyle modifications on sperm DNA fragmentation, 2025).
Oxidative stress — the underlying driver
Most sperm quality problems trace back to one thing: oxidative stress. Sperm cells are particularly vulnerable to free radical damage because they carry very little cytoplasm (and therefore fewer built-in antioxidant defences). When reactive oxygen species overwhelm the body's antioxidant capacity, the result is damage to sperm membranes, motility, and — critically — the DNA they carry.
This is why antioxidant-rich nutrition and targeted supplementation feature so prominently in the evidence. You're not just boosting a number on a test — you're protecting the integrity of the genetic material your baby will inherit.
Supplements That Actually Have Evidence Behind Them
I'm always cautious about supplement recommendations. The fertility supplement market is enormous, and much of it runs ahead of the science. But for male fertility, the evidence base is genuinely stronger than many people realise. A comprehensive 2025 meta-analysis of 50 randomised controlled trials found that while no single supplement reliably improved pregnancy rates on its own, specific nutrients did improve individual sperm parameters significantly (Nutrients, 2025).
Here's what the research supports:
CoQ10 (200–400 mg/day)
This is the one I'd start with. Coenzyme Q10 is a potent antioxidant that plays a direct role in mitochondrial energy production — and sperm need enormous amounts of energy to function. A 2024 meta-analysis of RCTs found that CoQ10 supplementation significantly improved sperm concentration, motility, and seminal CoQ10 levels, with better results at higher doses (400 mg outperformed 200 mg) and treatment durations over three months (Frontiers in Pharmacology, 2024). I've written extensively about CoQ10 for egg quality — the mechanism for sperm is remarkably similar.
Zinc (15–30 mg/day)
Zinc is essential for testosterone production, sperm membrane stability, and protecting DNA from oxidative damage. Seminal fluid contains higher concentrations of zinc than almost any other body tissue. Deficiency is linked to reduced sperm count and testosterone levels (Colagar et al., 2009). Most men in the UK get enough from food if their diet is varied, but if your partner's diet is heavy on processed foods and light on shellfish, red meat, seeds, and legumes, supplementation is worth considering.
Selenium (55–200 mcg/day)
Selenium works synergistically with other antioxidants — particularly when combined with N-acetylcysteine (NAC). The 2025 meta-analysis found selenium improved both sperm concentration and motility. Brazil nuts are one of the richest natural sources (just two to three daily can meet your selenium needs), but supplemental forms work too.
Omega-3 fatty acids (DHA, 500–1,000 mg/day)
DHA is a major structural component of the sperm cell membrane. Higher DHA intake is associated with improved morphology and motility. A 2019 trial found that omega-3 supplementation for 32 weeks improved sperm count, concentration, and morphology compared to placebo (Safarinejad, 2011). If your partner doesn't eat oily fish at least twice a week, supplementation makes sense. I cover the broader fertility benefits in my omega-3 and fertility guide.
L-Carnitine / Acetyl-L-Carnitine (1–3 g/day)
Carnitines are involved in fatty acid transport within mitochondria — essentially fuelling sperm motility. The evidence for carnitine is strongest when combined with other antioxidants. One meta-analysis found that carnitine plus vitamins was the most effective intervention for improving spontaneous pregnancy rates in subfertile men (Zheng et al., 2021).
Vitamin D (1,000–2,000 IU/day)
Vitamin D receptors are present throughout the male reproductive tract, and deficiency is associated with lower sperm motility and count. Given that most people in the UK are deficient during winter months, this is a sensible baseline supplement for everyone — not just those trying to conceive.
What about multis and branded fertility supplements?
Products like ConceptionXR, FertilAid, and Proxeed combine several of the above nutrients. They're convenient but often under-dosed on the ingredients that matter most (especially CoQ10, which is expensive to include at therapeutic levels). I'd rather you built a targeted stack based on evidence than relied on a one-size-fits-all capsule that ticks marketing boxes.
What He Eats Matters: Nutrition for Sperm Health
Supplements fill gaps, but they can't compensate for a poor diet. The dietary pattern with the strongest evidence for male fertility is — unsurprisingly — the Mediterranean diet. A 2017 systematic review found consistent associations between Mediterranean-style eating and better semen quality parameters (Salas-Huetos et al., 2017).

What does that look like in practice?
Plenty of oily fish (salmon, mackerel, sardines for omega-3s and vitamin D), colourful vegetables and berries (antioxidants), nuts and seeds (zinc, selenium, vitamin E), olive oil as the primary fat source, whole grains and legumes, and moderate amounts of poultry and eggs. The foods to minimise are the usual suspects: ultra-processed foods, excessive red and processed meat, sugary drinks, and trans fats.
I'd also add that fertility-supportive foods aren't complicated or expensive. Tinned sardines, frozen berries, pumpkin seeds, eggs — this isn't about buying high-end supplements. It's about consistently building meals from nutrient-dense whole foods. I talk about this a lot because it matters: food first, supplements second.
Lifestyle Changes That Make a Measurable Difference
This is where men have genuine, fast-acting leverage over their fertility. Unlike genetic factors or age-related decline, lifestyle modifications can produce visible improvements within a single spermatogenesis cycle.

Heat exposure
The testes sit outside the body for a reason — sperm production requires a temperature 2–4°C below core body heat. Anything that raises scrotal temperature for extended periods can impair spermatogenesis. A 2016 study found that daily hot baths significantly increased sperm cell death and DNA damage (Rao et al., 2016). Hot tubs, saunas, heated car seats, and prolonged laptop use on the lap are all worth reconsidering.
The encouraging part? The effects are reversible. Research shows sperm parameters return to normal within approximately six months of removing heat exposure (Shefi et al., 2007).
Smoking
The evidence here is unambiguous. Smoking reduces sperm count, motility, and morphology while increasing DNA fragmentation. A meta-analysis of 57 studies found that smokers had 13–17% lower sperm concentration and 10% lower motility compared to non-smokers (Sharma et al., 2016). Cannabis use carries similar risks — THC has been shown to reduce sperm concentration and alter morphology.
Alcohol
Moderate drinking (under 14 units per week) doesn't appear to dramatically affect sperm quality in most studies. But heavy or binge drinking is clearly harmful — it reduces testosterone production, impairs spermatogenesis, and increases oxidative stress. If your partner is a regular drinker, cutting back to a few drinks per week during the three months before trying to conceive is sensible.
Weight and exercise
Excess body fat increases oestrogen levels (through aromatisation of testosterone) and raises scrotal temperature. A BMI above 30 is associated with reduced sperm count and increased DNA fragmentation. Regular moderate exercise — 30 minutes most days — improves hormonal balance, blood flow, and antioxidant capacity. But there's a caveat: excessive endurance training and cycling (particularly on narrow saddles for extended periods) can have the opposite effect by raising scrotal temperature and compressing blood flow.
Sleep
This one gets overlooked. A 2020 study found that men who slept fewer than six hours per night had significantly lower sperm concentration compared to those sleeping seven to eight hours (Chen et al., 2020). Testosterone production peaks during sleep, so chronic sleep deprivation directly undermines the hormonal environment sperm need to develop.
Stress
Cortisol and testosterone have an inverse relationship — when stress hormones are chronically elevated, testosterone production drops. This isn't about telling your partner to "just relax" (that advice helps nobody). It's about recognising that sustained work pressure, fertility anxiety, and relationship strain all have biological consequences. I've written about the anxiety side of this in detail because it matters far more than people give it credit for.
Medications and Medical Conditions That Affect Sperm
Some fertility problems have medical causes that lifestyle alone won't fix. These need clinical attention.
Varicocele
A varicocele is an enlargement of the veins within the scrotum — essentially varicose veins of the testicle. It's the most common identifiable cause of male infertility, found in roughly 35–40% of men with primary infertility. Varicoceles raise scrotal temperature and increase oxidative stress. Surgical repair (varicocelectomy) has the strongest evidence of any intervention for reducing sperm DNA fragmentation (Scientific Reports, 2025).
Testosterone replacement therapy (TRT)
This is something every man considering fertility needs to know: exogenous testosterone shuts down sperm production. It's one of the most common iatrogenic causes of male infertility I come across. When the body receives testosterone externally, it reduces its own production of FSH and LH — the hormones that drive spermatogenesis. If your partner is on TRT, he needs to speak with his doctor about alternatives before trying to conceive. Recovery is possible but can take six to twelve months after stopping.
Other medications to flag
SSRIs, finasteride (used for hair loss), anabolic steroids, and some blood pressure medications can all impair sperm production or function. A medication review with a GP or fertility specialist is a sensible step if conception isn't happening as expected.
Clomiphene citrate (off-label)
Originally developed for female ovulation induction, clomiphene is increasingly prescribed off-label for men with low sperm counts. It works by stimulating the pituitary gland to produce more FSH and LH, which in turn drives testosterone and sperm production. Case reports include men going from severely low counts to clinically normal parameters within three months (though larger trials are still needed).
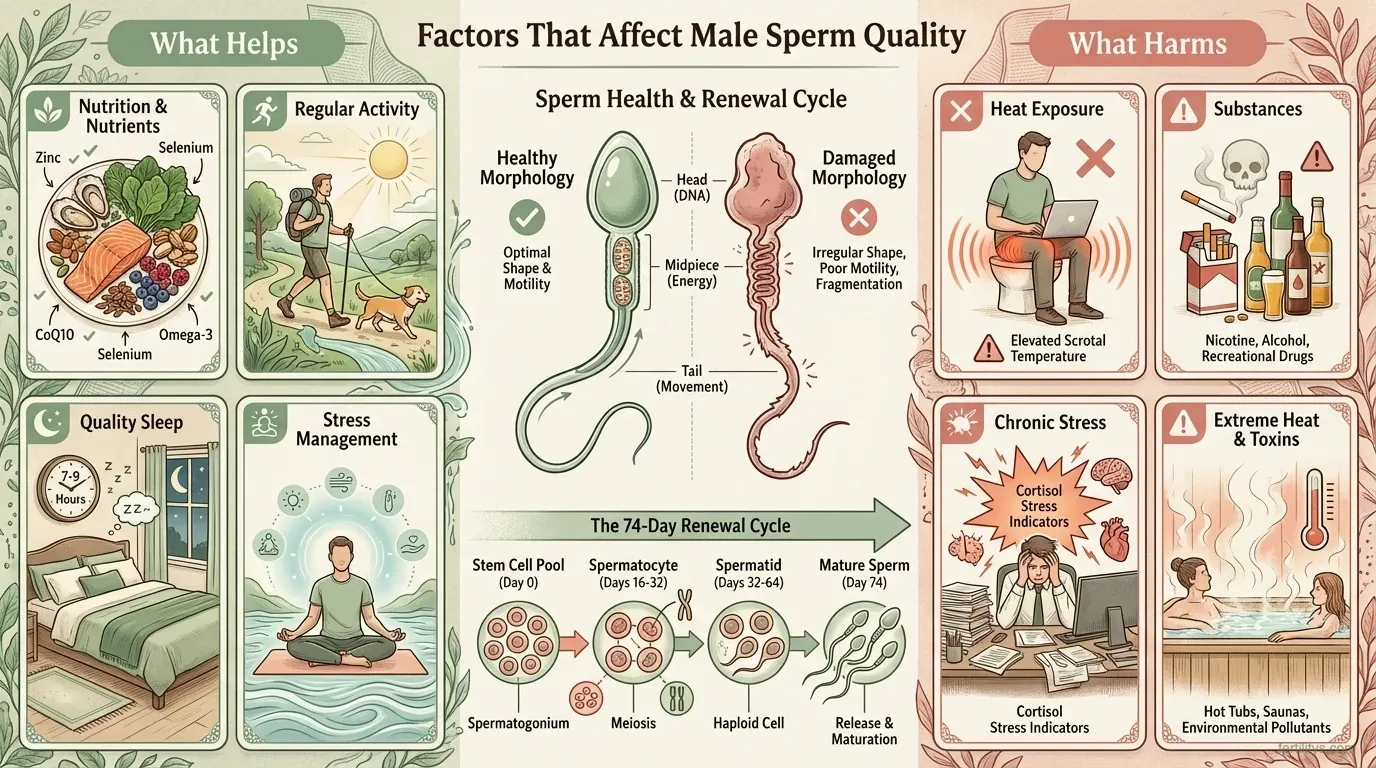
The 74-Day Rule: Why You Need to Give It Three Months
This is the single most important concept in male fertility improvement, and it's the one I hammer home with every couple I work with. Spermatogenesis — the complete cycle of sperm production from stem cell to mature spermatozoon — takes approximately 74 days, followed by another 10–14 days of maturation in the epididymis (Amann, 2008).
That means the sperm your partner produces today were already developing 10–12 weeks ago. Any change you make — whether it's starting a supplement, quitting smoking, improving diet, or reducing heat exposure — won't show up in a semen analysis for at least three months.
I know that feels like a long time when you're anxious to see progress. But flip it around: every positive change you make today is already protecting the sperm that will matter three months from now. Start now, be consistent, and don't judge the intervention by a test taken too early.
The Reddit fertility communities are full of success stories tied to this exact timeframe — men going from below-range parameters to normal after three months of targeted changes. The biology backs it up.
When Your Partner Won't Get Tested
I'm including this section because it's one of the most common frustrations I hear from women in their fertility journey — and it rarely gets addressed in clinical guides.
Male reluctance around fertility testing is real and deeply rooted. For many men, fertility feels tangled up with masculinity, virility, and identity. The idea that something might be "wrong" with their sperm touches nerves that go far beyond the clinical result. Add in the awkwardness of producing a sample in a clinic, and avoidance becomes an easy default.
What I've found works better than pressure is information. Share this article. Explain the 74-day window. Frame it not as "there might be something wrong with you" but as "we can actively improve our chances if we know where we stand." A male fertility test doesn't have to start at a clinic. At-home semen analysis kits (like the YO Sperm Test or ExSeed) can be a good entry point for men who aren't ready for a clinic visit. They're not a replacement for a full laboratory analysis, but they can lower the barrier to that first conversation.
And if results do come back suboptimal — remember that male infertility is not a character flaw. It's a medical finding, often temporary, and almost always improvable.
Making Fertility a Team Effort
One of the most important shifts I made in my own journey was moving from "my fertility" to "our fertility." When I was deep in my AMH results and building my supplement protocol, it was easy to feel like I was carrying the whole project. But the truth is that conception requires two healthy gametes meeting at the right time — and both partners have meaningful influence over the quality of what they bring.
If you're the one doing all the tracking, all the supplementing, and all the reading (and let's be honest, if you've read this far, that's probably you) — bring your partner into the process. Cook the Mediterranean meals together. Take the supplements at the same time. Go for the evening walk. Make it something you're both doing, rather than something being done to one of you.
For a practical starting point, my complete guide to getting pregnant covers timing, tracking, and what both partners can do to optimise the process.
The Bottom Line
Male fertility isn't fixed or mysterious. Sperm quality is dynamic — it responds to what you eat, how you live, what supplements you take, and what toxins you avoid. The 74-day spermatogenesis cycle means meaningful improvement is possible within three months of making targeted changes.
If you're wondering how to increase sperm count or improve motility, start with the basics: a semen analysis for a baseline, an honest audit of diet and lifestyle, and evidence-based supplements (CoQ10, zinc, selenium, omega-3s) given time to work. Address heat exposure, smoking, excess alcohol, and sleep quality. And if results don't improve after three to six months of consistent effort, seek a referral to a reproductive urologist or fertility specialist — because some causes (varicocele, hormonal imbalances, genetic factors) need clinical intervention.
Half of all fertility journeys involve a male factor. The sooner both partners engage with that reality, the sooner you can start making progress together.
Frequently Asked Questions
How long does it take to improve sperm quality?
Sperm take approximately 74 days to develop, with another 10–14 days of maturation. Most experts recommend allowing a full three months before retesting after making lifestyle or supplement changes. Some improvements in motility may appear earlier, but count and morphology changes need the full cycle.
Can you improve sperm morphology naturally?
Yes, to a degree. Morphology is influenced by oxidative stress, heat exposure, and toxin exposure. Antioxidant supplementation (particularly CoQ10 and vitamin E), quitting smoking, and reducing alcohol intake can improve morphology scores over three to six months. That said, morphology measured under strict Kruger criteria is the least predictive parameter for natural conception — so a low score alone isn't necessarily cause for alarm.
What is a normal sperm count?
According to the WHO 6th edition (2021), the 5th centile reference values are ≥16 million sperm per millilitre and ≥39 million total per ejaculate. These are lower-range thresholds — most fertile men produce significantly more. A count below these values warrants investigation but doesn't automatically mean infertility.
Does CoQ10 help male fertility?
The evidence is strong. A 2024 meta-analysis of randomised controlled trials found that CoQ10 significantly improved sperm concentration, motility, and clinical pregnancy rates. Higher doses (400 mg/day) outperformed lower doses, and treatment for longer than three months produced the best results. It's one of the most well-supported male fertility supplements available.
Can heat really damage sperm?
Yes. The testes need to be 2–4°C below core body temperature for optimal sperm production. Regular hot baths, saunas, hot tubs, and prolonged laptop use on the lap can raise scrotal temperature enough to impair spermatogenesis and increase DNA damage. The good news: these effects are reversible within roughly six months of removing the exposure.
Should my partner take a male fertility supplement?
If his diet is already excellent and varied, he may not need one. But most men in the UK don't consistently get optimal levels of zinc, selenium, CoQ10, and omega-3s from food alone — especially if their diet leans heavily on processed foods. A targeted supplement stack based on the evidence (rather than a generic fertility multi) is the approach I'd recommend.
What is sperm DNA fragmentation and should we test for it?
Sperm DNA fragmentation (SDF) measures damage to the genetic material inside sperm. A standard semen analysis doesn't assess this. High SDF is linked to failed IVF cycles, recurrent miscarriage, and unexplained infertility. If you've experienced any of these, requesting an SDF test from a private clinic or reproductive urologist is worth considering.
References
- Kumar, N. & Singh, A.K. (2015). Trends of male factor infertility, an important cause of infertility: A review of literature. Journal of Human Reproductive Sciences, 8(4), 191–196. doi:10.4103/0974-1208.170370
- World Health Organization. (2021). WHO laboratory manual for the examination and processing of human semen, 6th ed. Geneva: WHO. who.int
- National Institute for Health and Care Excellence. (2025). Fertility problems: assessment and treatment. NICE guideline CG156 (updated). nice.org.uk
- Hotaling, J.M. et al. (2012). Impact of strict sperm morphology on IUI and IVF outcomes. Human Reproduction, 27(7), 1967–1974.
- Agarwal, A. et al. (2020). Sperm DNA fragmentation: A new guideline for clinicians. The World Journal of Men's Health, 38(4), 412–471. doi:10.5534/wjmh.200128
- Nutrients. (2025). The effect of dietary supplements on male infertility in terms of pregnancy, live birth, and sperm parameters: A systematic review and meta-analysis. Nutrients, 17(10), 1710. PubMed
- Frontiers in Pharmacology. (2024). Does coenzyme Q10 improve semen quality and circulating testosterone level? A systematic review and meta-analysis of randomized controlled trials. PubMed
- Colagar, A.H. et al. (2009). Zinc levels in seminal plasma are associated with sperm quality in fertile and infertile men. Nutrition Research, 29(2), 82–88.
- Salas-Huetos, A. et al. (2017). Dietary patterns, foods and nutrients in male fertility parameters and fecundability: a systematic review of observational studies. Human Reproduction Update, 23(4), 371–389. doi:10.1093/humupd/dmx006
- Rao, M. et al. (2016). Experimental mild increase in testicular temperature has drastic, but reversible, effect on sperm quality. Translational Andrology and Urology.
- Shefi, S. et al. (2007). Improvement of semen quality after lifestyle changes in infertile men. Fertility and Sterility.
- Sharma, R. et al. (2016). Cigarette smoking and semen quality: a new meta-analysis. European Urology, 70(4), 635–645. doi:10.1016/j.eururo.2016.04.010
- Chen, Q. et al. (2020). Sleep deprivation may impair semen quality. Sleep, 43(Supplement 1).
- Amann, R.P. (2008). The cycle of the seminiferous epithelium in humans: A need to revisit? Journal of Andrology, 29(5), 469–487.
- Zheng, D. et al. (2021). Effects of medicines and supplements on spontaneous pregnancy and semen parameters in male infertility: A systematic review update and network meta-analysis. Engineering, 7(4). doi:10.1016/j.eng.2020.11.011
Cite this page
Bowen, D. (2026). Male fertility: How to improve sperm quality naturally. Fertilitys. https://fertilitys.com/getting-pregnant/male-fertility-improve-sperm-quality-naturally/
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. The content is based on published research and written by Danielle Bowen MSc RNutr, but it should not replace consultation with your GP, fertility specialist, or healthcare provider. If you have concerns about male fertility, please speak with a qualified medical professional.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











