How to Get Pregnant: A Nutritionist's Complete Preconception Guide
Everything you need to know about getting pregnant — from fertile window timing and age-by-age statistics to the 12-month preconception plan that changed my own fertility journey.


When I decided I was ready to start trying, I assumed it would happen quickly. I was healthy, I ate well, I exercised. I thought I'd be pregnant within a couple of months. That's not what happened.
What I learned — through my own journey and through years of working with fertility clients — is that getting pregnant isn't just about having sex at the right time. It's about the months of preparation beforehand. The nutritional foundations you lay. The lifestyle changes that improve egg quality. The things nobody tells you until you're already struggling.
This guide is everything I wish someone had told me before I started trying. Not the oversimplified "just relax and it'll happen" advice. The actual, evidence-based, practical steps that genuinely improve your chances of conceiving — whether you're planning ahead or already in the middle of trying.
Understanding Your Fertile Window
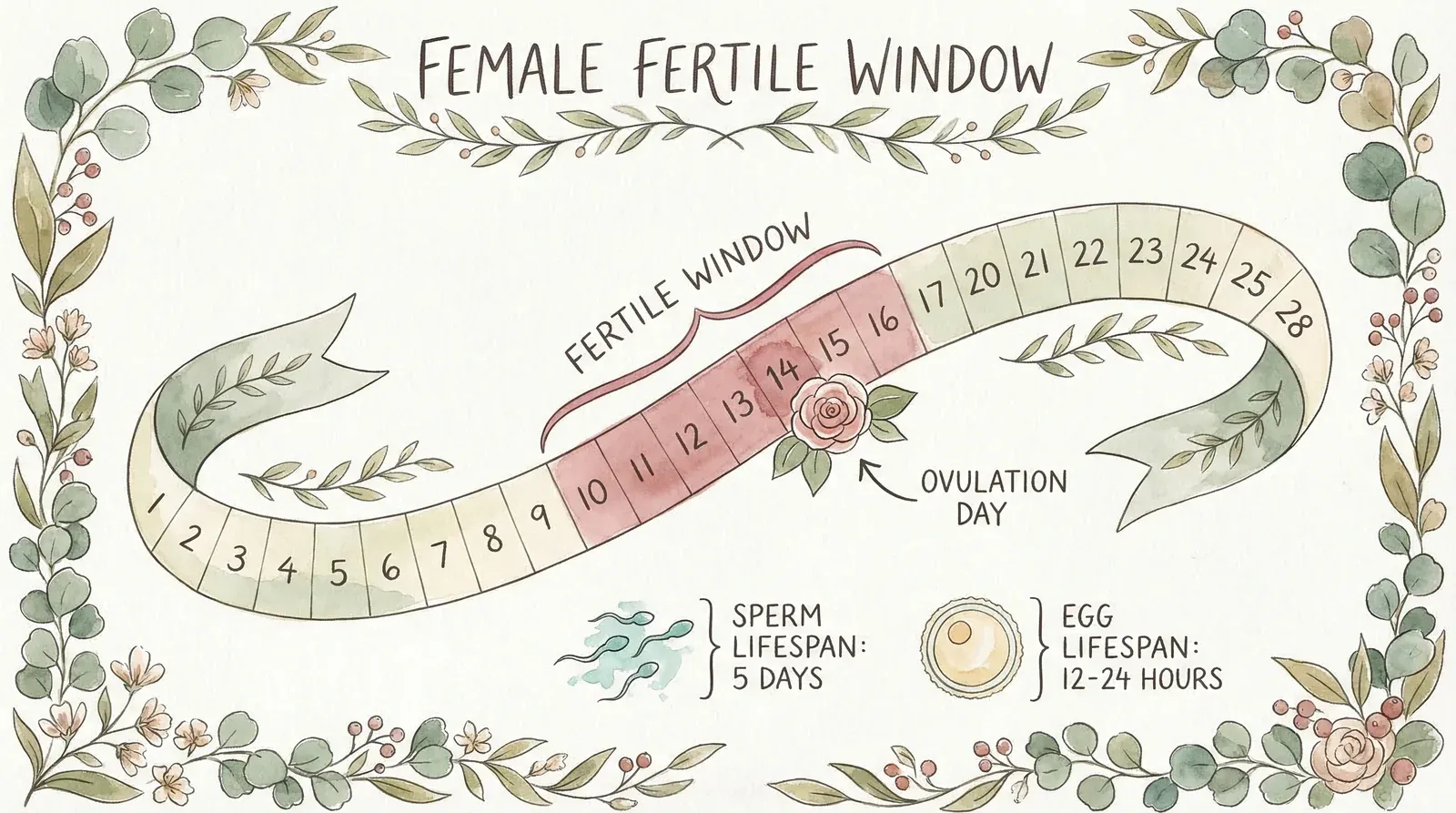
Every month, you have approximately six days when conception is possible. That's it. Six days out of an entire cycle. If you miss this window, no amount of perfectly timed sex will result in pregnancy that month.
The fertile window is the five days before ovulation plus ovulation day itself. Here's why: sperm can survive in the female reproductive tract for up to five days (Wilcox et al., 1995, New England Journal of Medicine), but your egg lives for only 12-24 hours after release. So the ideal scenario is having sperm already waiting in the fallopian tubes when your egg is released.
The day-by-day conception probabilities, based on Wilcox et al.'s landmark study of 221 healthy women, look like this:
| Day Relative to Ovulation | Probability of Conception |
|---|---|
| 5 days before | ~4% |
| 4 days before | ~8% |
| 3 days before | ~15% |
| 2 days before | ~25% |
| 1 day before (peak) | ~28% |
| Ovulation day | ~10% |
| Day after ovulation | ~0% |
Notice something surprising? The day before ovulation has the highest conception rate — not ovulation day itself. By the time you ovulate, the window is already closing. This is why tracking methods that only tell you "you've ovulated" are less useful than ones that predict ovulation in advance.
How to Track Your Fertile Window
There are several evidence-based methods, and combining them gives you the best picture:
- Ovulation predictor kits (OPKs) — detect the LH surge that occurs 24-36 hours before ovulation. The most practical method for most women. Start testing from around cycle day 10 (or 3-4 days before you expect your LH surge).
- Basal body temperature (BBT) — your temperature rises by 0.2-0.5°C after ovulation due to progesterone. The catch: it only confirms ovulation after it's happened, so it's retrospective. Useful for confirming you're ovulating but not great for predicting the current cycle's window.
- Cervical mucus monitoring — as you approach ovulation, your cervical mucus becomes clear, stretchy, and slippery (like raw egg white). This "fertile-quality" mucus helps sperm travel and survive. When you notice it, you're likely in your fertile window.
- Fertility monitors — devices like the Inito, Mira, or Clearblue Advanced monitor that track multiple hormones (LH, oestrogen, progesterone, PdG) for a more complete picture. I've reviewed several of these on the site.
My practical advice? Start with simple OPKs for two to three cycles to learn your pattern. If your cycles are irregular or you want more data, consider upgrading to a hormone-tracking monitor. But don't overthink it — many women conceive just by having regular sex every 2-3 days throughout their cycle, without tracking anything.
How Often Should You Have Sex?
This question comes up in almost every preconception consultation I do. The evidence is clearer than most people think:
- Every 1-2 days during the fertile window gives the best chance of conception (NICE, 2013; Gaskins et al., 2018)
- Every 2-3 days throughout your cycle if you're not tracking ovulation — this ensures you never miss the window entirely
- Daily sex is fine — it doesn't significantly deplete sperm count in most men. A 2004 WHO study confirmed that sperm parameters remained normal even with daily ejaculation over 5 days.
- Abstaining for long periods is counterproductive — beyond 5 days of abstinence, sperm DNA fragmentation increases (Levitas et al., 2005, Fertility and Sterility)
And a note on timing: you don't need to have sex at specific times of day, or lie with your legs in the air afterwards (that's a myth — sperm reach the cervical mucus within seconds). Just have sex regularly during your fertile window and try not to turn it into a chore. Easier said than done, I know.
Your Chances of Conceiving by Age
I'm going to give you the real numbers here, because I think women deserve honest information rather than vague reassurances. These figures come from a 2017 prospective cohort study of 2,962 women (Wesselink et al., American Journal of Epidemiology):
| Age | Chance per Cycle | Within 6 Months | Within 12 Months |
|---|---|---|---|
| Under 25 | ~25% | ~63% | ~85% |
| 25-27 | ~23% | ~59% | ~79% |
| 28-30 | ~22% | ~62% | ~78% |
| 31-33 | ~20% | ~55% | ~74% |
| 34-36 | ~17% | ~46% | ~66% |
| 37-39 | ~13% | ~38% | ~55% |
| 40+ | ~7-10% | ~25-30% | ~40-45% |
A few things I want you to take away from this:
- The decline is gradual, not a cliff. There's no magic age where fertility suddenly drops off — it's a steady decline that accelerates after 35.
- Even at 37-39, over half of women conceive within a year. The statistics aren't as bleak as headlines suggest.
- These are population averages. Your individual fertility depends on ovarian reserve, hormonal balance, lifestyle factors, and your partner's sperm quality — not just your age.
- You can influence several of these factors. Age you can't change. But egg quality, hormonal balance, and nutritional status? Those respond to intervention. That's what the rest of this article covers.
I was 32 when I started trying, with an AMH of 3 (expected for my age: 20+). By the numbers, my chances looked grim. But with the right preparation — which took me nearly a year — I conceived naturally. The statistics matter, but they're not the whole story.
The 12-Month Preconception Plan
This is what separates my approach from most fertility advice you'll read online. Most sources tell you to "start trying" and maybe take folic acid. I tell my clients to start preparing their bodies at least a year before actively trying to conceive. Not three months — a year.
Here's why: your eggs take approximately 90 days to mature from dormant follicle to ovulation-ready egg. So the egg you ovulate this month started its development three months ago — and was influenced by your nutrition, stress levels, toxin exposure, and supplement status during that entire window. If you start preconception supplements the month you start trying, you've already missed three cycles' worth of eggs.
Starting 12 months out gives you:
- Time to identify and address any underlying issues (hormone imbalances, nutrient deficiencies, thyroid problems)
- Three to four complete egg maturation cycles under optimised conditions before you actively try
- Time for lifestyle changes to genuinely take effect — supplement levels don't reach therapeutic levels overnight
- A buffer for the unexpected — maybe your vitamin D is severely low (takes 3-6 months to correct), or you discover you have PCOS

Months 12-9: Foundations
- Book a preconception health check — blood tests for thyroid (TSH, fT4), vitamin D, iron/ferritin, B12, folate, AMH (ovarian reserve), and a basic hormone panel. Your GP should do these — push for them if they're reluctant.
- Start a prenatal supplement — at minimum: 400mcg folic acid (or 400mcg methylfolate if you have MTHFR variants), vitamin D (10mcg/day per NHS guidelines, I personally take more), omega-3 DHA (at least 200mg/day for brain development). Don't wait until you're pregnant — start NOW.
- Address any chronic health issues — get your thyroid optimised (TSH between 1-2.5 for conception, not just "in range"), manage blood sugar if needed, deal with any dental issues (gum disease is linked to preterm birth).
- Start reducing environmental toxins — switch to clean beauty products, avoid BPA (canned food linings, plastic containers), reduce exposure to pesticides. I did a full audit of my bathroom cabinet and kitchen at this stage.
Months 9-6: Nutrition and Lifestyle
- Adopt a Mediterranean-style fertility diet — the Nurses' Health Study II (Chavarro et al., 2007, Obstetrics & Gynecology) found that women following a "fertility diet" had a 66% lower risk of ovulatory infertility. Focus on: whole grains, full-fat dairy, plant proteins alongside animal protein, iron-rich foods, and abundant vegetables.
- Add fertility-specific supplements — CoQ10 (200mg/day for egg quality — Ben-Meir et al., 2015), vitamin D to sufficiency, omega-3 if not eating oily fish 2-3x/week.
- Optimise your exercise routine — moderate exercise supports fertility. Excessive exercise (particularly high-intensity training) can disrupt ovulation. I stopped HIIT entirely and switched to yoga, walking, and gentle strength training. A 2012 study found that moderate exercise was associated with improved fertility, while vigorous exercise was associated with reduced fertility in normal-weight women (Wise et al., Fertility and Sterility).
- Manage stress — easier said than done, I know. But cortisol directly suppresses reproductive hormones (GnRH, LH, FSH). Find what works for you: yoga, meditation, acupuncture (I did fertility acupuncture weekly), walking in nature, therapy. Build it into your routine now, not when you're already stressed about conceiving.
- Cut alcohol — I went completely alcohol-free during my preconception year. The evidence on moderate alcohol and fertility is mixed, but a 2021 Danish cohort study of 6,120 women found that even moderate drinking (1-6 drinks per week) was associated with reduced fecundability (Mikkelsen et al., Human Reproduction).
- Stop recreational drugs — cannabis, cocaine, and MDMA all have documented negative effects on both egg and sperm quality. This is non-negotiable.
Months 6-3: Fine-Tuning
- Start cycle tracking — learn your pattern over 3+ cycles before actively trying. Use OPKs, BBT, or a fertility monitor. Note your cycle length, when you ovulate, and your luteal phase length (ideally 12-14 days).
- Get your partner involved — sperm quality matters just as much. He should also be taking supplements (zinc, selenium, CoQ10, folic acid), cutting back on alcohol, avoiding hot baths/saunas, keeping his laptop off his lap, and wearing loose boxers. Sperm take 74 days to develop, so he needs at least 3 months of preparation too.
- Dental check-up — deal with any gum disease now (it's linked to preterm birth and low birth weight)
- Review medications — some common medications can affect fertility (certain antidepressants, anti-inflammatories, antihistamines that dry cervical mucus). Talk to your GP about switching if needed. Do NOT stop prescribed medications without medical advice.
Month 3 Onwards: Active Trying
- Have regular sex — every 1-2 days during your fertile window, or every 2-3 days throughout your cycle
- Keep taking your supplements — don't stop now
- Try to enjoy it — I know that sounds hollow when you're anxious, but stress genuinely affects hormones. Do whatever helps you stay present rather than treating sex as a medical procedure.
- Don't test too early — implantation typically occurs 6-12 days post-ovulation. Testing before 12 DPO gives unreliable results and unnecessary heartbreak. I've written detailed guides for each day in the two-week wait.
🍎 Go Organic With the Dirty Dozen
These twelve fruits and vegetables carry the heaviest pesticide loads. I tell all my clients: if you can only afford to go organic on some things, make it these. The rest you can buy conventional and wash well.
The list: Strawberries, spinach, kale/collard/mustard greens, peaches, pears, nectarines, apples, grapes, bell & hot peppers, cherries, blueberries, green beans (EWG, 2025).
Preconception Nutrition: What to Eat (and What to Avoid)
This is my area of expertise, and it's where I believe most women can make the biggest difference to their fertility. The research on preconception nutrition has exploded in the last decade, and the evidence is now clear: what you eat in the months before conception matters — for your fertility, for your pregnancy, and for your baby's long-term health.
The Fertility Diet
The most robust evidence comes from the Nurses' Health Study II — a prospective study that followed 17,544 women over 8 years. The researchers identified a dietary pattern associated with a 66% lower risk of ovulatory infertility (Chavarro et al., 2007). The key components:
- Plant protein alongside animal protein — replacing some animal protein with plant sources (lentils, chickpeas, beans, nuts) was associated with improved ovulatory function
- Full-fat dairy — counter-intuitively, full-fat dairy was associated with better fertility outcomes than low-fat. One serving of full-fat dairy per day was linked to a 27% lower risk of ovulatory infertility.
- Complex carbohydrates — whole grains, sweet potato, legumes instead of refined carbs and sugar
- Iron from plants and supplements — non-heme iron intake was inversely associated with ovulatory infertility risk
- Healthy fats — monounsaturated (olive oil, avocado) and omega-3 fats. Minimise trans fats (partially hydrogenated oils).
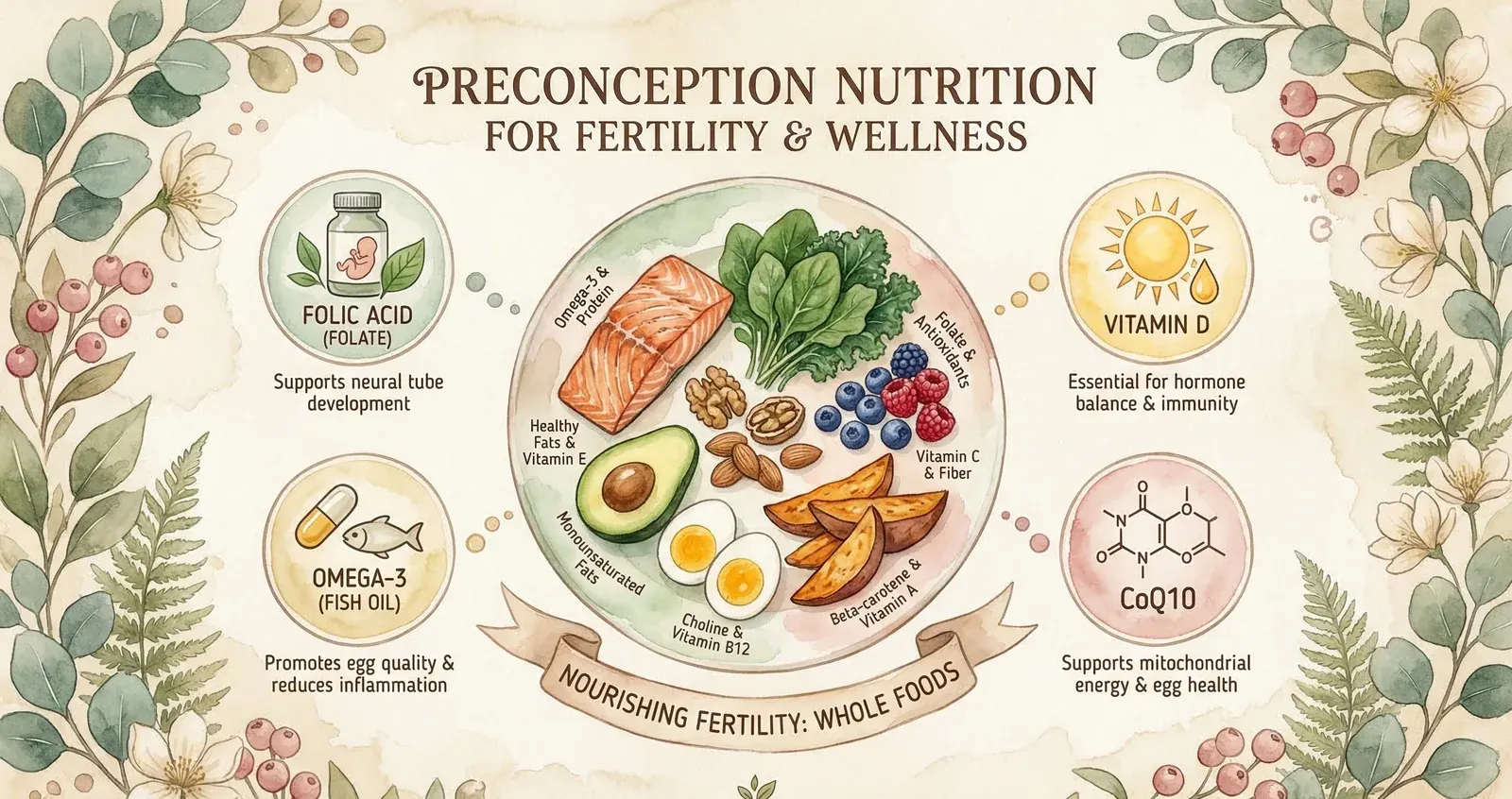
Foods to Prioritise
- Oily fish 2-3x/week — salmon, sardines, mackerel. Rich in omega-3 DHA/EPA. A 2018 study found women who consumed more seafood had higher fecundability (Gaskins et al., Journal of Clinical Endocrinology & Metabolism).
- Leafy greens daily — folate, iron, calcium, antioxidants. Spinach, kale, broccoli, rocket.
- Eggs — choline (critical for neural tube development — most women don't get enough), plus high-quality protein and vitamin D.
- Berries — antioxidant powerhouses. Blueberries, strawberries (organic — they're on the dirty dozen list), raspberries.
- Nuts and seeds — walnuts (omega-3), Brazil nuts (selenium — 1-2 per day for thyroid support), pumpkin seeds (zinc), flaxseed (lignans for hormone balance).
- Full-fat natural yoghurt — probiotics for gut health, calcium, protein. Choose plain over flavoured.
- Extra virgin olive oil — your primary cooking fat. Anti-inflammatory, rich in polyphenols.
Foods to Reduce or Avoid
- Alcohol — I went completely dry. Even moderate intake (1-6 drinks/week) is associated with reduced fecundability.
- Caffeine — limit to 200mg/day (roughly 1-2 cups of coffee). Higher intake has been associated with longer time to pregnancy (Buck Louis et al., 2016).
- Ultra-processed foods — associated with increased inflammation and insulin resistance, both of which impair fertility.
- Trans fats — each 2% increase in trans fat intake was associated with a 73% increase in ovulatory infertility in the Nurses' Health Study.
- Excess sugar — drives insulin resistance, which disrupts ovulation. This is especially important if you have PCOS.
- High-mercury fish — avoid swordfish, shark, king mackerel, tilefish. Mercury is a reproductive toxin.
Essential Supplements for Conception
Even with a perfect diet, certain nutrients are nearly impossible to get in sufficient quantities from food alone during the preconception period. Here's what the evidence supports:
| Supplement | Dose | Why It Matters | Start When |
|---|---|---|---|
| Folic acid / Methylfolate | 400-800mcg/day | Prevents neural tube defects. 70% of NTDs could be prevented with adequate folate (AJOG, 2008). Start BEFORE conception — the neural tube closes by week 4. | 12 months before |
| Vitamin D | 10-25mcg (400-1000 IU)/day | Deficiency is linked to reduced fertility and higher miscarriage risk. A 2018 meta-analysis found vitamin D sufficiency improved IVF outcomes by 34% (Chu et al., Human Reproduction). | 12 months before |
| Omega-3 (DHA) | 200-500mg DHA/day | Critical for baby's brain and eye development. Also reduces inflammation and supports egg quality. | 12 months before |
| CoQ10 | 200mg/day | Supports mitochondrial function in eggs. A 2024 meta-analysis found improved clinical pregnancy rates with CoQ10 supplementation (Xu et al., Annals of Medicine). | 6-12 months before |
| Iron | Only if deficient | Low ferritin is linked to anovulation and longer time to pregnancy. Test first — don't supplement blindly. | As needed |
| Iodine | 150mcg/day | Essential for thyroid function and baby's brain development. UK diets are often deficient. | 3-6 months before |
I personally took: folic acid (methylfolate, 800mcg), vitamin D (25mcg/day — I was deficient), CoQ10 (200mg as ubiquinol), omega-3 (fish oil, 1g with 500mg DHA), a Wild Nutrition fertility multivitamin, and magnesium glycinate (300mg at night). That was my stack for about 10 months before we started trying. I've written a full breakdown of my supplement protocol in my supplements guide.
Lifestyle Factors That Affect Fertility
Nutrition and supplements get the most attention, but your broader lifestyle has an equally powerful effect on your fertility.

Exercise: The Goldilocks Zone
Moderate exercise supports fertility. Vigorous exercise can impair it. A 2012 prospective cohort study of 3,628 Danish women found that vigorous exercise (running, fast cycling, gymnastics) was associated with reduced fecundability in normal-weight women, while moderate exercise (brisk walking, leisurely cycling, gardening) was associated with improved outcomes (Wise et al., 2012, Fertility and Sterility).
What I recommend to my clients:
- Walking 30+ minutes daily — especially after meals for blood sugar regulation
- Yoga 2-3x/week — I did fertility yoga specifically. It combines gentle physical movement with stress reduction.
- Strength training 2x/week — builds muscle, which improves insulin sensitivity
- Avoid excessive HIIT, heavy running, or CrossFit — especially if you have irregular cycles. I was doing intense HIIT 4-5x/week before my fertility journey and my acupuncturist told me to stop immediately. She was right.
Sleep
Aim for 7-9 hours of consistent sleep. Disrupted sleep patterns affect melatonin production (which is a powerful antioxidant in the ovarian follicle) and elevate cortisol, which suppresses reproductive hormones. Night shift work has been specifically linked to menstrual irregularity and longer time to pregnancy (Lawson et al., 2011, Occupational and Environmental Medicine).
My sleep routine during preconception: bed by 10pm, phone away by 9pm, bedroom completely dark, magnesium glycinate 30 minutes before sleep. I also wore blue-light blocking glasses in the evening — the evidence is emerging, but melatonin production is sensitive to light exposure.
Stress Management
I hesitate to include this because "just relax" is the most infuriating advice anyone can give to someone trying to conceive. But the biology is real: chronic stress elevates cortisol, which suppresses GnRH (the hormone that triggers LH and FSH release), which disrupts ovulation.
A 2014 prospective study of 501 couples found that women with the highest biomarkers of stress (salivary alpha-amylase) took 29% longer to conceive compared to those with the lowest stress levels (Lynch et al., Human Reproduction). That's not "just relax" — it's evidence that stress-reduction strategies genuinely help.
What helped me: weekly fertility acupuncture, daily walks in nature, yoga, reducing my work schedule, and — honestly — therapy. Having someone to process the anxiety with made a real difference.
Environmental Toxins
Endocrine disruptors (chemicals that interfere with your hormones) are everywhere, and their effects on fertility are increasingly well-documented:
- BPA and phthalates — found in plastics, food can linings, receipts, personal care products. Switch to glass containers, BPA-free options, and clean beauty products.
- Pesticides — a 2018 study in JAMA Internal Medicine found that women who consumed the most pesticide-contaminated produce had 26% lower odds of clinical pregnancy during IVF (Chiu et al.). Buy organic where possible — especially the dirty dozen.
- Heavy metals — mercury (high-mercury fish), lead (old paint, some cosmetics), cadmium (cigarette smoke). Test your levels if you have known exposure.
I did a complete audit of my home during preconception. I switched my shampoo, deodorant, moisturiser, cleaning products, and cooking pans. Extreme? Maybe. But these chemicals accumulate over time, and the preconception period is when you want to minimise your body's toxic load.
Your Partner's Role (It's 50% of the Equation)

Half the genetic material comes from your partner. Half. Yet most fertility advice is directed exclusively at women. Male factor contributes to approximately 40-50% of all infertility cases (Agarwal et al., 2021, The Lancet).
What He Should Be Doing
- Taking supplements — zinc (15-30mg/day), selenium (55-100mcg/day), CoQ10 (200mg/day), folic acid (400mcg/day), and vitamin C (500mg/day). A 2020 Cochrane review found that antioxidant supplementation in men improved pregnancy rates.
- Keeping cool — sperm production requires a temperature 2-4°C below body temperature. Avoid hot baths, saunas, tight underwear, and laptops directly on the lap.
- Cutting alcohol and smoking — both significantly reduce sperm count, motility, and morphology. Even moderate alcohol intake affects sperm quality.
- No recreational drugs — cannabis in particular is associated with reduced sperm count and motility.
- Exercising moderately — regular exercise improves sperm parameters. Excessive exercise (like marathon training) can have the opposite effect.
- Getting a semen analysis — if you've been trying for 6+ months without success, a semen analysis is a simple, non-invasive test that can identify issues early. Many couples spend months (and money) investigating the female partner first, when a £50 semen analysis could have identified the problem immediately.
Tim — my partner — was brilliant about this. He took supplements from the same time I did, cut back on alcohol, and got his semen analysis done early. Not every partner will be as proactive, but having the conversation early matters. This is a team effort.
When to Seek Help
The standard advice is to see a fertility specialist if you haven't conceived after:
- 12 months of regular unprotected sex if you're under 35
- 6 months if you're 35 or over
- Immediately if you have known risk factors: irregular or absent periods, history of PID or STIs, endometriosis, PCOS, previous surgery on your reproductive organs, or known male factor issues
But here's what I tell my clients: don't wait the full 12 months if something feels wrong. If your cycles are irregular, if you're not detecting ovulation on OPKs, if your periods are extremely heavy or painful — see your GP now. You don't need to "qualify" for investigation by trying for a year first.
Tests Your GP Should Run
If you do seek help, here's the panel you should push for:
- Day 2-3 blood tests: FSH, LH, oestradiol, AMH (ovarian reserve), thyroid function (TSH, fT4), prolactin
- Day 21 progesterone (or 7 days after expected ovulation) — confirms whether you're ovulating
- Pelvic ultrasound — checks ovarian follicle count, uterine structure, and rules out fibroids/polyps
- Semen analysis for your partner — counts, motility, morphology, volume
- STI screening — chlamydia in particular can cause tubal damage without symptoms
- Tubal patency test (HyCoSy or HSG) — if initial tests are normal but you're still not conceiving, checking whether your fallopian tubes are open is the next step
Common Myths About Getting Pregnant
"Just relax and it'll happen"
While stress does affect fertility (see above), telling someone to "just relax" ignores the biological, nutritional, and medical factors that also play a role. Nobody tells a man with low sperm count to "just relax." This advice is dismissive, gendered, and usually wrong.
"You can't get pregnant on your period"
Unlikely but not impossible — especially if you have short cycles. If you ovulate on day 10 and have sex on day 5 (still bleeding), sperm could survive the 5 days and be present at ovulation.
"Certain positions improve your chances"
No evidence supports this. Sperm reach the cervical mucus within seconds of ejaculation regardless of position. Have sex in whatever position is comfortable and enjoyable.
"You should lie with your legs up afterwards"
A 2009 randomised trial in the BMJ actually tested this (in the context of IUI) and found 15 minutes of immobilisation slightly improved pregnancy rates — but this was during a clinical procedure, not natural intercourse. For natural conception, there's no evidence that lying down afterwards makes any meaningful difference.
"Organic food doesn't matter"
The 2018 JAMA Internal Medicine study I mentioned earlier found a significant association between pesticide-contaminated produce consumption and reduced fertility. It may not matter for everyone, but for women actively trying to conceive, reducing pesticide exposure — especially from the dirty dozen — is a reasonable precaution backed by evidence.
If you're trying to get pregnant, understanding your cycle is the single most impactful thing you can do to increase your chance of getting pregnant. Timing intercourse around ovulation — when the egg travels from the ovary through the fallopian tube toward the womb — gives sperm the best opportunity to reach and fertilise the egg. The fertile window includes the five days before ovulation and the day of ovulation itself, because sperm can survive in the reproductive tract (including the cervix and vagina) for up to five days.
Maintaining a healthy weight is another factor that significantly affects fertility for both partners. Research consistently shows that a BMI between 19 and 25 is associated with the highest natural conception rates. Being significantly over or underweight can disrupt ovulation, reduce sperm quality, and make it harder to become pregnant. If you've been using contraception, most methods allow fertility to return within one to three cycles — though hormonal injections may take longer.
The Bottom Line
Getting pregnant is a combination of biology, timing, nutrition, and — yes — some luck. You can't control everything, but you can control far more than most people realise.
Start early. Give yourself at least a year of preparation if you can. Get your bloods done, optimise your nutrition, take the right supplements, move your body gently, manage your stress, and involve your partner from day one. These aren't marginal gains — they're the foundations that give you the best possible chance.
And if it doesn't happen as quickly as you hoped? That's not failure. It's normal. The average healthy couple under 30 still has only a 20-25% chance per cycle. Give yourself grace, get the right investigations done, and know that there are many paths to parenthood — and most of them lead somewhere good.

You might also find helpful:
▸How long does it usually take to get pregnant?
For a healthy couple under 30, there's about a 20-25% chance of conceiving per cycle, with 85% conceiving within 12 months. At 35, about 66% conceive within a year. At 40+, around 40-45% conceive within 12 months. These are averages — individual factors like ovarian reserve, sperm quality, and overall health can significantly affect your timeline.
▸What is the best time to have sex to get pregnant?
The 5 days before ovulation and ovulation day itself — a 6-day window. The highest conception probability is the day before ovulation (~28%). Having sex every 1-2 days during this window gives the best chance. If you're not tracking ovulation, having sex every 2-3 days throughout your cycle ensures you won't miss the window.
▸What should I eat to boost my fertility?
Follow a Mediterranean-style diet: oily fish 2-3x/week, abundant vegetables and leafy greens, full-fat dairy, whole grains, nuts and seeds, extra virgin olive oil, and plant proteins alongside animal protein. The Nurses' Health Study II found this pattern reduced ovulatory infertility risk by 66%. Reduce ultra-processed foods, trans fats, excess sugar, and limit caffeine to 200mg/day.
▸What supplements should I take before trying to conceive?
At minimum: folic acid or methylfolate (400-800mcg/day — start 3-12 months before trying), vitamin D (10-25mcg/day), and omega-3 DHA (200-500mg/day). For egg quality support, add CoQ10 (200mg/day). Only supplement iron if blood tests show you're deficient. A good prenatal multivitamin covers most bases, but check the dosages — many are underdosed.
▸Does age affect male fertility too?
Yes. While men can technically father children at older ages, sperm quality (count, motility, morphology, and DNA integrity) declines from around age 40. Paternal age over 40 is associated with longer time to conception, increased miscarriage risk, and slightly higher rates of certain conditions in offspring. Both partners should optimise their health before trying.
▸When should I see a doctor if I'm not getting pregnant?
See your GP after 12 months of regular unprotected sex if you're under 35, or after 6 months if you're 35 or over. See them immediately if you have irregular periods, known PCOS or endometriosis, a history of pelvic infections, or known male factor issues. Don't wait if something feels wrong — you don't need to "qualify" for investigation.
▸Can you get pregnant on your period?
It's unlikely but possible, particularly if you have short cycles. If you ovulate early (e.g., day 10) and have sex towards the end of your period (e.g., day 5-6), sperm could survive the 4-5 days and be present when you ovulate. For most women with regular 28-30 day cycles, the risk is very low.
References
- Wilcox AJ et al. (1995). Timing of sexual intercourse in relation to ovulation. New England Journal of Medicine, 333(23):1517-1521. doi:10.1056/NEJM199512073332301
- Wesselink AK et al. (2017). Age and fecundability in a North American preconception cohort study. American Journal of Epidemiology, 187(12):2540-2551. doi:10.1093/aje/kwy188
- Chavarro JE et al. (2007). Diet and lifestyle in the prevention of ovulatory disorder infertility. Obstetrics & Gynecology, 110(5):1050-1058. doi:10.1097/01.AOG.0000287293.25465.e1
- Ben-Meir A et al. (2015). Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell, 14(5):887-895. doi:10.1111/acel.12368
- Wise LA et al. (2012). A prospective cohort study of physical activity and time to pregnancy. Fertility and Sterility, 97(5):1136-1142. doi:10.1016/j.fertnstert.2012.02.025
- Lynch CD et al. (2014). Preconception stress increases the risk of infertility. Human Reproduction, 29(5):1067-1075. doi:10.1093/humrep/deu032
- Mikkelsen EM et al. (2021). Alcohol consumption and fecundability. Human Reproduction, 31(4):751-758. doi:10.1093/humrep/dew021
- Gaskins AJ et al. (2018). Seafood intake, sexual activity, and time to pregnancy. Journal of Clinical Endocrinology & Metabolism, 103(7):2680-2688. doi:10.1210/jc.2018-00385
- Levitas E et al. (2005). Relationship between the duration of sexual abstinence and semen quality. Fertility and Sterility, 83(6):1680-1686. doi:10.1016/j.fertnstert.2004.12.045
- Chiu YH et al. (2018). Association between pesticide residue intake from consumption of fruits and vegetables and pregnancy outcomes among women undergoing infertility treatment. JAMA Internal Medicine, 178(1):17-26. doi:10.1001/jamainternmed.2017.5038
- Agarwal A et al. (2021). Male infertility. The Lancet, 397(10271):319-333. doi:10.1016/S0140-6736(20)32667-2
- Lawson CC et al. (2011). Rotating shift work and menstrual cycle characteristics. Occupational and Environmental Medicine, 68(3):168-174.
- Chu J et al. (2018). Vitamin D and assisted reproductive treatment outcome: a systematic review and meta-analysis. Human Reproduction, 33(1):65-80. doi:10.1093/humrep/dex326
- Xu Y et al. (2024). Coenzyme Q10 in reproductive disorders. Annals of Medicine, 56(1):2312372.
Medical Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider about your fertility and preconception health. Individual results vary — the information here reflects current evidence and my clinical experience as a registered nutritionist, not a guarantee of outcomes. Danielle Bowen is a registered nutritionist (RNutr), not a medical doctor.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











