Ectopic Pregnancy: Symptoms, Causes, and What Happens Next
What an ectopic pregnancy means, how it's treated, and what it means for your fertility — from a nutritionist who understands pregnancy loss.


Key Takeaways
- Around 90% of ectopic pregnancies occur in the fallopian tube — the rest implant on the ovary, cervix, caesarean scar, or abdomen
- Sharp one-sided pain and vaginal bleeding between weeks 4 and 12 are the most common warning signs
- Ectopic pregnancies can't be moved to the uterus — they always need treatment
- Three treatment paths exist: expectant management (watchful waiting), methotrexate injection, or surgery
- Between 50 and 80% of women conceive again within two years of an ectopic pregnancy
Nobody plans for this. You see a positive pregnancy test, and for a few hours — maybe a few days — you let yourself imagine. Names. Due dates. How you'll tell people.
And then something shifts. A sharp pain that doesn't feel right. Bleeding that's different from spotting. A scan that shows an empty uterus when there should be something there.
An ectopic pregnancy is one of the most frightening things that can happen in early pregnancy. It's also more common than most people realise, and the medical care around it is better than it's ever been. This article covers what happens, how it's diagnosed, what treatment looks like, and what it means for your fertility going forward — because that's usually the first question.
What Is an Ectopic Pregnancy?
In a typical pregnancy, a fertilised egg travels down the fallopian tube and implants in the uterine lining. In an ectopic pregnancy, the embryo implants somewhere outside the uterus — a location where it can't grow into a baby and, if left untreated, can become dangerous.
The word "ectopic" simply means "out of place." It's not something you did wrong. It's not caused by stress or exercise or that glass of wine before you knew. In most cases, there's no clear single cause — just a combination of factors that slowed the embryo's journey or altered the tubal environment.
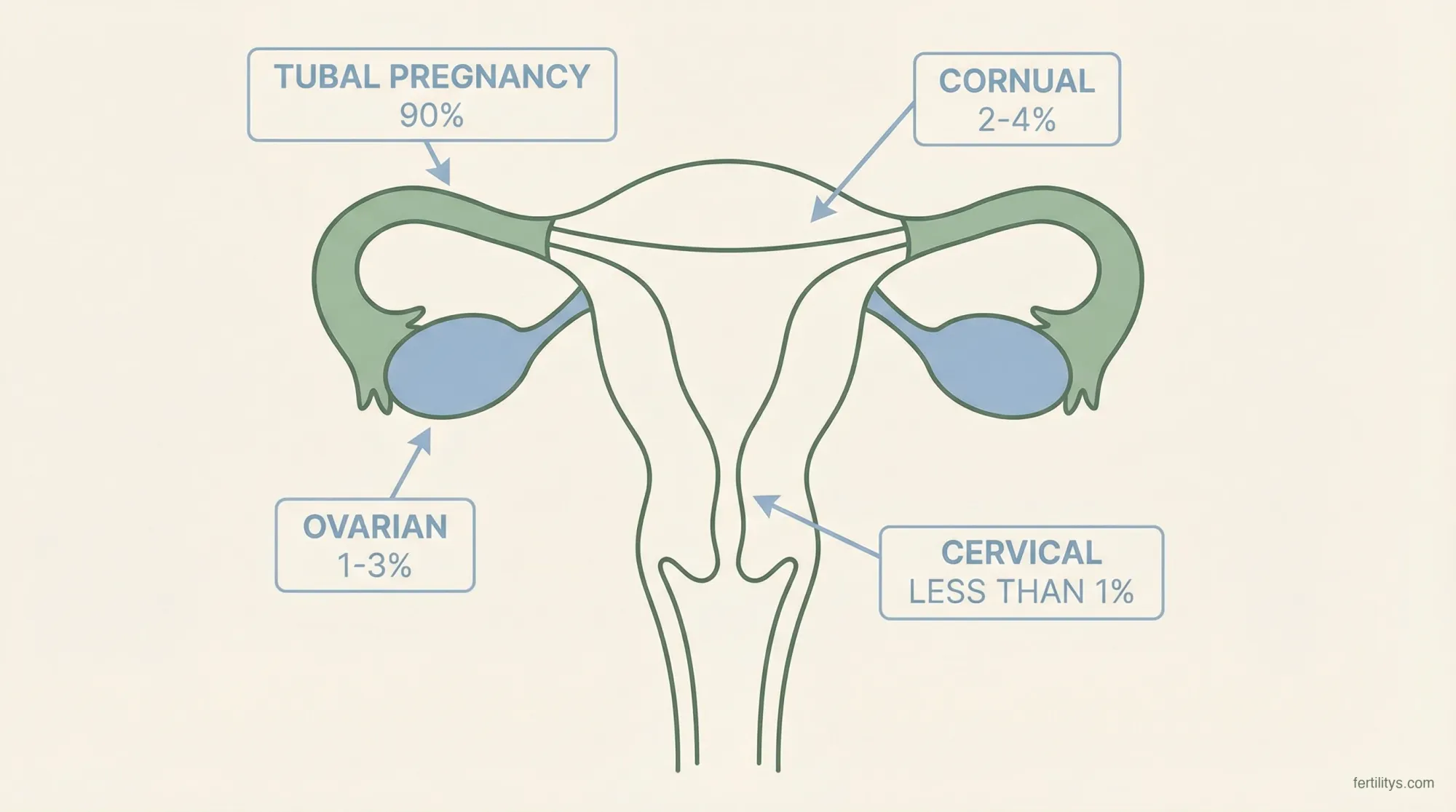
Where ectopic pregnancies happen:
- Fallopian tube — about 90% of all ectopic pregnancies, most commonly in the ampulla (the wider section nearest the ovary). This is known as a tubal pregnancy
- Ovary — roughly 1–3% of ectopic pregnancies
- Caesarean scar — becoming more common as C-section rates rise (around 4–9% in some studies)
- Cervix — rare, less than 1%
- Abdomen — very rare, but documented
- Interstitial (cornual) — where the tube meets the uterus, around 2–4%. Harder to detect and more dangerous because this area has a richer blood supply
A heterotopic pregnancy — where one embryo implants in the uterus and another in the tube simultaneously — is exceptionally rare in natural conception (about 1 in 30,000) but more common with IVF, occurring in roughly 1 in 100 assisted pregnancies (Statpearls, 2025).
The pregnancy can never be saved or transplanted to the uterus. This is a fact, not a failure — it's simply the biology. And understanding that early can help you make sense of the treatment decisions ahead.
Who Is at Higher Risk?
Any woman who can get pregnant can have an ectopic pregnancy. But certain factors increase the risk significantly. A 2024 systematic review and meta-analysis by Brim et al., published in the International Journal of Gynaecology and Obstetrics, pooled data from over 25,000 patients and identified these key risk factors (Brim et al., 2025):
Strongest risk factors:
- Previous ectopic pregnancy — 9× higher risk (OR 9.03). This is the single biggest predictor
- Pelvic inflammatory disease (PID) — 4× higher risk (OR 4.00). Usually caused by untreated chlamydia or gonorrhoea, PID creates scar tissue inside the tubes
- Previous abdominal or pelvic surgery — 5.6× higher risk (OR 5.60). Any surgery that involves the pelvis can create adhesions
- Previous tubal ligation — 5.6× higher risk (OR 5.59). If pregnancy occurs after sterilisation, it's significantly more likely to be ectopic
- History of infertility — 3.7× higher risk (OR 3.70)
Moderate risk factors:
- Smoking — damages the cilia (tiny hairs) that help transport the egg through the tube
- Maternal age over 35 (and particularly over 40 — OR 1.46)
- Current IUD use — IUDs are excellent at preventing pregnancy, but the rare pregnancies that do occur with an IUD in place have a higher chance of being ectopic
- History of sexually transmitted infections, even if treated
- IVF and assisted reproduction — slightly elevated risk, particularly with embryo transfer
Endometriosis, previous miscarriage, and use of emergency contraception also appear in the literature, though with weaker associations. The overall risk of ectopic pregnancy is higher in women undergoing fertility treatment, particularly IVF with embryo transfer. But many women with ectopic pregnancies have none of these risk factors at all.
Symptoms of an Ectopic Pregnancy
This is the section I want you to really read — because early detection changes everything. The Ectopic Pregnancy Trust reports that all 12 maternal deaths from ectopic pregnancy in the UK during 2020–22 could have had better care, and improvements might have changed the outcome for nine of those women.
Ectopic symptoms usually appear between weeks 4 and 12 of pregnancy, though some women have no symptoms at all until a rupture.
Early warning signs:
- One-sided abdominal or pelvic pain — often sharp, sometimes cramping, different from period pain. It may come and go or be constant
- Vaginal bleeding — different from a period. Often darker, more watery, and may start and stop
- Shoulder tip pain — pain where your shoulder meets your arm. This sounds odd, but it's caused by internal bleeding irritating the diaphragm. It's a red flag
- Pain when using the toilet — particularly when opening your bowels
- Feeling faint or dizzy
If a tube ruptures (a medical emergency):
- Sudden, severe abdominal pain
- Feeling very faint, dizzy, or like you might collapse
- Looking very pale
- Rapid heartbeat
- Feeling sick or vomiting
If you recognise these symptoms, call 999 (UK) or 911 (US) immediately. A ruptured ectopic is a life-threatening emergency that requires surgery.
One reason ectopic pregnancies can be missed is that the symptoms overlap with other conditions — urinary tract infections, gastroenteritis, chemical pregnancy, or a miscarriage. NICE guidelines (NG126) recommend that any woman of childbearing age presenting with abdominal pain should have a pregnancy test, specifically because of this overlap (NICE, 2023).
How Ectopic Pregnancy Is Diagnosed
Diagnosis usually involves a combination of blood tests and ultrasound — sometimes over several days, which can feel agonising when you're worried.
Blood hCG levels — Human chorionic gonadotropin (hCG) is the pregnancy hormone measured by home pregnancy tests. In a healthy pregnancy, hCG roughly doubles every 48 hours during the first weeks. In an ectopic pregnancy, levels often rise more slowly or plateau. Your doctor will likely check hCG on two occasions, 48 hours apart, to see the trend.
Transvaginal ultrasound — This is the primary diagnostic tool. An ultrasound can usually detect a pregnancy in the uterus by around 5–6 weeks (when hCG reaches roughly 1,500–2,000 IU/L). If hCG levels suggest pregnancy but no intrauterine pregnancy is visible, your team will investigate further.
Sometimes, the ultrasound directly shows a mass in the tube. Other times, it simply shows an empty uterus with rising hCG — this is called a pregnancy of unknown location (PUL), and it means more monitoring is needed before a definitive diagnosis.
The waiting during this diagnostic phase is brutal. You're pregnant, but you don't know where. You can't plan. You can't relax. If you're in this limbo right now — I'm sorry. It's one of the hardest parts, and your feelings about it are completely valid.
Treatment Options
Treatment depends on several factors: how far along the pregnancy is, your hCG levels, whether there are symptoms, and whether the tube has ruptured. NICE guideline NG126 outlines three approaches (NICE, 2023).
Expectant Management (Watchful Waiting)
In some cases — when hCG levels are low and falling on their own, there's no significant pain, and no sign of rupture — doctors may recommend monitoring without active treatment. The body resolves the pregnancy naturally in some cases. This requires regular blood tests and close follow-up, and it's only appropriate when the clinical picture is very specific.
Methotrexate
Methotrexate is an injection that stops the pregnancy cells from growing. It's given when the ectopic is confirmed but hasn't ruptured, hCG levels are below a certain threshold (typically under 5,000 IU/L, though protocols vary), and the ectopic mass is relatively small.
After the injection, you'll need regular blood tests to confirm hCG levels are dropping. It can take several weeks for levels to return to zero. Side effects can include nausea, tiredness, and abdominal discomfort. You'll need to avoid alcohol and folic acid supplements during treatment and wait at least three months before trying to conceive again — methotrexate can affect egg quality and folate metabolism.
A narrative review of long-term outcomes found the pooled rate of subsequent intrauterine pregnancy after methotrexate was 69.6%, with a recurrent ectopic rate of about 10% (Medical and Pharmacological Sciences, 2025).
Surgery
Surgery is necessary when the tube has ruptured, symptoms are severe, hCG levels are high, or other treatments aren't appropriate. Two surgical approaches exist:
Salpingotomy — the tube is opened, the ectopic tissue is removed, and the tube is repaired. This preserves the tube but carries a small risk (around 8%) that some ectopic tissue remains, requiring further treatment.
Salpingectomy — the affected tube is completely removed. This is more common when the tube is significantly damaged. Losing one tube doesn't mean you can't get pregnant — you still ovulate from both ovaries, and the remaining tube can collect eggs from either side.
Both procedures are usually done laparoscopically (keyhole surgery), which means smaller incisions and faster recovery. Emergency surgery for a rupture may require open surgery (laparotomy) depending on the situation.
Fertility After Ectopic Pregnancy
This is the question that sits behind everything else. Can I still have a baby?
The answer, for most women, is yes.
Research published in Biomedicines (2025) found that between 50 and 80% of women who try to conceive following an ectopic pregnancy become pregnant again within two years, assuming there are no other significant fertility issues (Biomedicines, 2025).
Fertility outcomes depend on several things:
- How you were treated — methotrexate and salpingotomy generally preserve future fertility equally well. Salpingectomy reduces the chance slightly if the other tube also has issues, but many women with one tube conceive without difficulty
- Your other tube — if the remaining tube is healthy and open, natural conception is very possible
- The cause — if PID or tubal damage caused the ectopic, that underlying issue may affect future conception too
- Age — as with all fertility, age matters. Women under 35 generally have better outcomes
- Recurrence risk — about 10% of women who've had one ectopic will have another. This sounds daunting, but it also means 90% won't
If you've had an ectopic and are struggling to conceive afterwards, IVF bypasses the tubes entirely. It's a viable route if tubal damage is the barrier.
When I was going through my own fertility journey — two chemical pregnancies, the constant cycle of hope and loss — I learned something that stuck with me: your body's ability to conceive doesn't disappear because of one terrible experience. It might take longer. You might need more support. But the door isn't closed.
Emotional Recovery — the Part Nobody Talks About Enough
Ectopic pregnancy is a pregnancy loss. Full stop. You were pregnant, and now you're not, and some people will minimise that because "it was early" or "it wasn't viable."
Those people are wrong.
The emotional fallout from ectopic pregnancy can be as significant as the physical recovery — sometimes more so. Research consistently shows elevated rates of anxiety, depression, and symptoms of PTSD in the months following an ectopic pregnancy. Grief doesn't follow a timeline, and there's no "correct" way to feel. Some women feel relief that they're safe. Some feel devastated. Many feel both simultaneously.
What I see in practice, again and again, is that women feel pressure to "move on" before they're ready. Partners want to start trying again. Families offer well-meaning but painful advice. And there's often a deep fear that it'll happen again — a fear that can make subsequent pregnancies feel less joyful and more anxious.
Things that help:
- Give yourself permission to grieve at your own pace
- Connect with others who've been through it — the Ectopic Pregnancy Trust runs a support forum and helpline
- Ask about counselling through your GP or early pregnancy unit — many offer this, but you might need to request it
- If you're struggling with anxiety about trying again, that's completely normal and worth talking to someone about
- Know that in subsequent pregnancies, your doctor should offer an early scan (around 6 weeks) to confirm the pregnancy is in the right place. This provides enormous peace of mind
When to Seek Help
Call 999/911 immediately if you have:
- Sudden, severe abdominal pain
- Feeling faint, dizzy, or collapsing
- Shoulder tip pain combined with abdominal pain
- Signs of shock: rapid heartbeat, pale skin, confusion
See your GP or attend A&E if:
- You have a positive pregnancy test and one-sided pelvic pain
- You're bleeding vaginally and know you're pregnant
- You have risk factors and are experiencing any unusual pain or bleeding in early pregnancy
There's no "too cautious" with ectopic pregnancy. The earlier it's caught, the more treatment options you have and the better the outcome for your future fertility.
The Bottom Line
An ectopic pregnancy is a medical emergency that needs treatment — but it's not the end of your fertility story. Most women go on to conceive again, whether naturally or with assisted reproduction. What matters most is early detection, appropriate treatment, and giving yourself space to recover — physically and emotionally.
If you're reading this because you're worried right now: get checked. Don't wait. Don't google for another three hours. Call your early pregnancy unit, your GP, or go to A&E. The worst thing that can happen is they send you home reassured. And that's not a bad outcome at all.
▸Can an ectopic pregnancy move to the uterus?
No. Once an embryo has implanted outside the uterus, it cannot be relocated. There is currently no medical procedure that can transplant an ectopic pregnancy to the womb. The pregnancy must be treated to protect the mother's health.
▸How long after an ectopic pregnancy can you try again?
This depends on your treatment. After surgery, most doctors advise waiting two to three full menstrual cycles to allow healing. After methotrexate, the usual recommendation is at least three months, because the drug affects folate levels and could potentially impact early embryo development. After expectant management, you'll typically be advised to wait until hCG returns to zero and you've had one normal period.
▸Can you still get pregnant with only one fallopian tube?
Yes. You ovulate from both ovaries, and the remaining tube can pick up eggs from either side — a process called transperitoneal migration. Many women with one tube conceive naturally without difficulty. If the remaining tube is damaged, IVF bypasses the tubes entirely.
▸Does an ectopic pregnancy show on a home pregnancy test?
Yes — an ectopic pregnancy produces hCG just like a uterine pregnancy, so a home test will be positive. However, a home test can't tell you where the pregnancy is located. If you have a positive test and are experiencing pain or unusual bleeding, see a doctor.
▸What causes ectopic pregnancy to rupture?
As the embryo grows in the confined space of the fallopian tube, it eventually outgrows what the tube can accommodate. The tube stretches and eventually tears, causing internal bleeding. This typically happens between weeks 6 and 10, though timing varies. Rupture is a medical emergency requiring immediate surgery.
References
- Brim, A.C.S. et al. (2025). Risk factors for ectopic pregnancy occurrence: Systematic review and meta-analysis. International Journal of Gynaecology and Obstetrics, 168(3), 919–932. doi:10.1002/ijgo.15965
- NICE (2023). Ectopic pregnancy and miscarriage: diagnosis and initial management [NG126]. National Institute for Health and Care Excellence. nice.org.uk/guidance/ng126
- Ectopic Pregnancy Trust (2024). About ectopic pregnancy. Data sourced from MBRRACE-UK Confidential Enquiries into Maternal Deaths 2020–22. ectopic.org.uk
- StatPearls (2025). Ectopic Pregnancy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. ncbi.nlm.nih.gov/books/NBK539860
- Biomedicines (2025). After the Shock: Impact of Ectopic Pregnancy on Subsequent Fertility and Parenthood. Biomedicines, 13, 2205. PMC12467044
- Mayo Clinic Health System (2022). Ectopic pregnancy: Signs, treatment and future fertility. mayoclinichealthsystem.org
- BMJ (2000). Ectopic pregnancy. BMJ, 320(7239), 916. Incidence: 11.5 per 1,000 pregnancies in the UK. doi:10.1136/bmj.320.7239.916
⚕️ Medical Disclaimer
This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Ectopic pregnancy is a medical emergency that requires urgent care. Always seek the advice of your doctor or other qualified health professional with any questions you may have. If you are experiencing symptoms of ectopic pregnancy, contact your nearest emergency department immediately. Never delay seeking medical advice because of something you have read on this website.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











