Unexplained Infertility: What to Do When Everything Looks Fine
A nutritionist's guide to what the diagnosis really means, what tests you're missing, and what to do next


You've done everything right. I see this all the time in my practice. The blood tests, the scans, the awkward cup in a clinic bathroom. And the results came back… fine. All of them. Normal hormones, open tubes, good sperm count, confirmed ovulation. Your doctor smiles and says "everything looks great."
Except you're still not pregnant.
If you've been diagnosed with unexplained infertility, I want you to know something — and I always say this to my clients before we go any further: this diagnosis is not a dead end. It's a starting point — one that deserves more investigation, clearer thinking, and a plan that doesn't leave you staring at the ceiling at 2am wondering what's wrong with you.
In my experience, here's the truth the label doesn't tell you. "Unexplained" describes the limits of testing, not the absence of a problem. And there are real, evidence-based steps you can take right now.
📋 Key Takeaways
- 15–30% of infertility cases are classified as unexplained — it's one of the most common diagnoses
- "Unexplained" means standard tests didn't find a cause, not that nothing is wrong
- Up to 43% conceive without treatment, but active intervention (IUI, IVF) significantly improves those odds
- Additional testing — laparoscopy, DNA fragmentation, endometrial biopsy — can uncover causes the standard workup misses
- The emotional toll is real and clinically significant — mental health support should be part of your plan
What unexplained infertility actually means
Unexplained infertility is diagnosed when a couple has been trying to conceive for at least 12 months (or 6 months if the woman is over 35) and standard fertility investigations come back normal. According to the National Institute for Health and Care Excellence (NICE) and the European Society of Human Reproduction and Embryology (ESHRE), that standard workup should cover four things: ovulation status, tubal patency, semen analysis, and assessment of the uterine cavity (Raperport, 2026).
If all four check out, you get the label.
The problem? "Standard testing" is not "comprehensive testing." It's a first pass — the basics that rule out the most common and most obvious causes. It catches blocked tubes, absent ovulation, and very low sperm counts. But it misses an entire category of subtler issues that can absolutely prevent pregnancy.
StatPearls (updated April 2026) puts the prevalence at 15–30% of all infertility cases. In the UK, it accounts for roughly 25% of infertility diagnoses (PMC, 2023). That means if you're sitting in a waiting room with nine other couples dealing with infertility, two or three of you are probably hearing "we can't find anything wrong."
You're not rare. You're not unlucky. You're dealing with a diagnosis that, by its very nature, describes what we don't know rather than what we do.
Why "everything is normal" doesn't mean nothing is wrong
This is the part I wish every doctor took five extra minutes to explain. The standard fertility workup tests for:
- Ovulation — are you releasing an egg? (blood tests, ultrasound tracking)
- Tubal patency — are your tubes open? (hysterosalpingogram / HSG)
- Semen analysis — is there enough sperm, and do they move? (count, motility, morphology)
- Uterine cavity — is there anything physically blocking implantation? (ultrasound or hysteroscopy)
What it does not routinely test for:
- Sperm DNA fragmentation — a man can have a perfectly normal semen analysis but still have sperm with damaged DNA that prevents fertilisation or causes early embryo loss. Standard SA doesn't measure this (Aitken & Curry, 2011).
- Silent endometriosis — endometriosis can exist without any symptoms. No painful periods, no pain during sex, nothing. The only definitive diagnosis is laparoscopic surgery. Research suggests endo may be present in 25–50% of unexplained infertility cases (Brosens et al., 2013).
- Chronic endometritis — a low-grade bacterial infection of the uterine lining that interferes with implantation. Diagnosed via endometrial biopsy (EMMA/ALICE test). Treatable with antibiotics, but rarely checked in a standard workup.
- Immune factors — natural killer (NK) cell activity and other immune responses can theoretically interfere with implantation. Controversial and not universally accepted, but some clinics investigate after repeated failures.
- Uterine receptivity — the window of implantation can be displaced in some women. Tests like the ERA (Endometrial Receptivity Array) attempt to identify the optimal transfer timing.
So when your doctor says "everything is normal," what they really mean is: "the standard tests didn't find anything." That's not the same as "there's nothing to find."
I've worked with clients who spent two years accepting "unexplained" as a final answer. When they finally pushed for a laparoscopy, they discovered stage III endometriosis. One surgery later, they were pregnant within three months. The label had described the limits of the investigation — not the limits of their body.
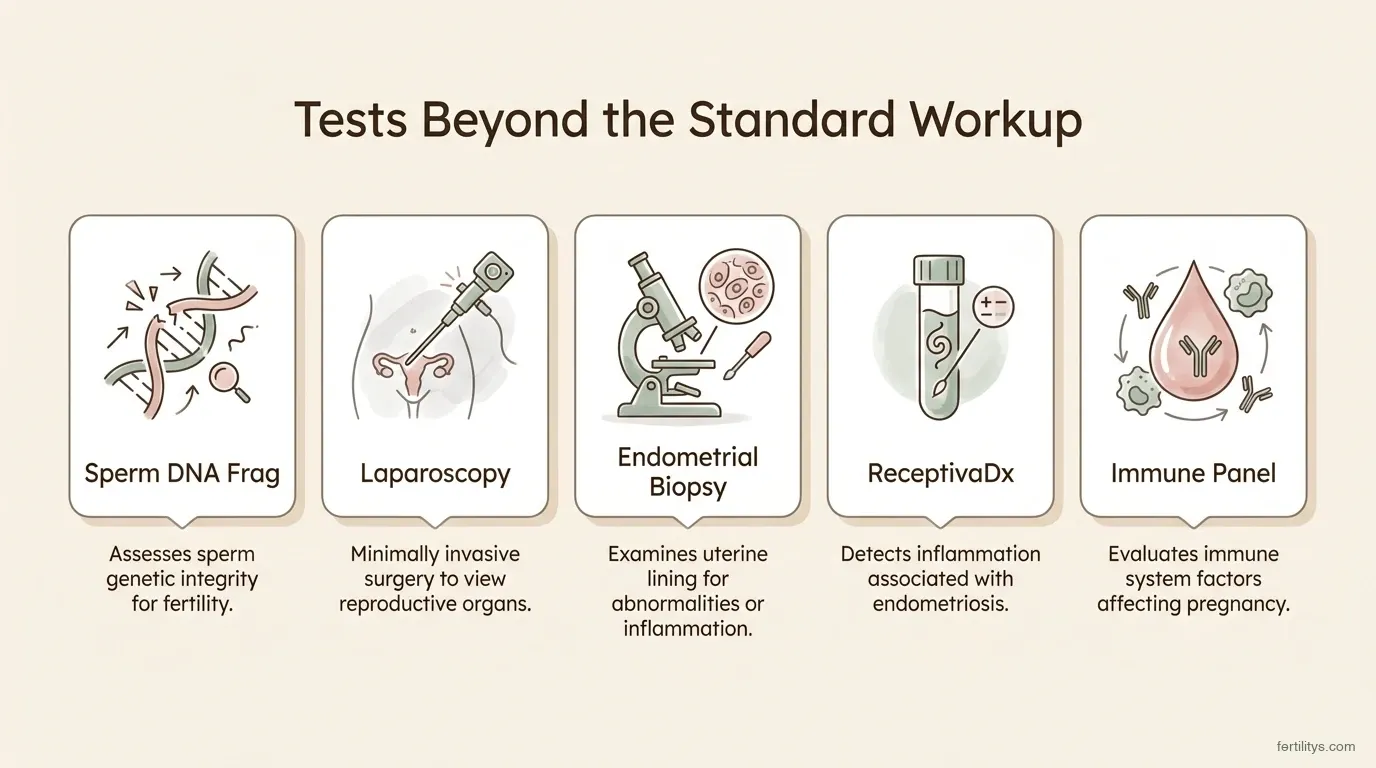
Five tests that go beyond the standard fertility workup — and can uncover hidden causes
Treatment options: from watchful waiting to IVF
One of the hardest things about unexplained infertility is that there's no single "fix." Treatment is a ladder — and where you start depends on your age, how long you've been trying, your finances, and your emotional capacity.
Expectant management (active monitoring)
Before you panic, there's genuinely good news here. A significant proportion of people with unexplained infertility conceive without any treatment at all. Cleveland Clinic cites research showing up to 43% eventually achieve pregnancy naturally. A study published in Human Reproduction found spontaneous conception rates of 13–15% in the first year after diagnosis, rising to around 35% over three years (Brandes et al., 2011).
Expectant management means continuing timed intercourse with lifestyle optimisation for a defined period — typically 6–12 months if you're under 35, shorter if you're older. It's not "doing nothing." It's a deliberate, evidence-informed choice that respects the biology of human conception (which, even under perfect conditions, is only about 20–25% per cycle).
IUI with ovarian stimulation
If expectant management hasn't worked, IUI (intrauterine insemination) with medication is usually the next step. The evidence here is fairly consistent: IUI with ovarian stimulation increases live birth rates roughly threefold compared to expectant management alone (Raperport, 2026; PMC review, 2023).
Per-cycle success rates for medicated IUI in unexplained infertility hover around 10–15%. Most specialists recommend trying up to three cycles — success rates plateau after that point, and if it hasn't worked by cycle three, it's time to consider escalating.
Medications used alongside IUI include letrozole (Femara), clomiphene citrate (Clomid), and gonadotropins. A cohort study cited by the ASRM found pregnancy rates of 34.7% with clomiphene and gonadotropin IUI versus 8.9% with expectant management (ASRM Practice Committee, 2020).
IVF
IVF offers the highest per-cycle success rates — around 40–50% depending on age and other factors. A 2024 individual participant data meta-analysis published in Human Reproduction found no robust evidence that IVF achieves pregnancy faster than IUI with ovarian stimulation, but IVF has a distinct advantage: it's both treatment and diagnostic tool.
That's important. IVF reveals things no blood test or scan can: whether your eggs fertilise normally, whether embryos develop to blastocyst, whether chromosomally normal embryos implant successfully. Many couples discover through IVF that their "unexplained" infertility actually had a clear biological cause — poor egg quality invisible on paper, fertilisation failure, or arrested embryo development.
NICE recommends offering IVF after two years of unsuccessful expectant management for couples with unexplained infertility. The 2023 ESHRE guideline supports IUI with ovarian stimulation as first-line, with IVF as the next step. The honest answer is that the right path depends on your specific situation — and a good fertility specialist will help you navigate that, not push you in one direction.
What you can do right now (while you're figuring out next steps)
Whether you're in the expectant management phase, between IUI cycles, or waiting for an IVF referral, there are evidence-based things you can do today.
Push for additional testing. Ask your doctor specifically about sperm DNA fragmentation testing, a laparoscopy for silent endometriosis, and endometrial biopsy for chronic endometritis. These three tests alone can uncover causes in a significant percentage of "unexplained" cases. If your doctor dismisses the request, consider a second opinion.
Optimise what you can control. A Mediterranean-style diet rich in fertility-supporting foods, omega-3 fatty acids, and folate has the strongest evidence base for fertility support (Karayiannis et al., 2018). CoQ10 (200–600mg daily) supports mitochondrial function in both eggs and sperm. Vitamin D deficiency — extremely common in the UK — is linked to implantation failure and should be tested and corrected if low.
Address lifestyle factors. Smoking, excessive alcohol, high BMI, and intense exercise (more than 7 hours per week of vigorous activity) are all associated with reduced fertility. These aren't guaranteed fixes, but they remove barriers.
Get your partner tested beyond the basics. If the standard semen analysis was the only male-side test, there's more to investigate. DNA fragmentation testing, oxidative stress assessment, and even lifestyle factors like heat exposure and cycling habits can all be relevant.
The emotional weight of not knowing
This section matters more than most of the medical information above, and I don't say that lightly.

A good fertility specialist will help you navigate options — not push you in one direction
Unexplained infertility carries a psychological burden that's different from other diagnoses. When you have PCOS, or endometriosis, or a specific male factor, you have something to point at. Something to research, treat, fight against. With no diagnosis, you're facing an invisible enemy — and the medical system has essentially told you "we don't know."
Research from the American Psychiatric Association reports that up to 40% of women experiencing infertility have a psychiatric diagnosis, most commonly depression or anxiety. Fewer than 7% seek professional mental health support. The distress is often amplified when there's no clear cause, because the absence of a diagnosis creates a vacuum that self-blame and anxiety rush to fill.
I've seen it in my own practice. Clients with unexplained infertility often describe it as worse than a diagnosis would be. At least then they'd have something concrete. Instead, they cycle through guilt ("maybe I'm too stressed"), suspicion ("maybe he's hiding something"), and despair ("maybe I'm just not meant to be a mum").
If this is you, please hear this: your feelings are valid, and getting professional support is not a sign of weakness — it's part of your treatment. Our guide to fertility anxiety covers coping strategies in more detail. A therapist who specialises in fertility can help you set boundaries around treatment decisions, manage the anxiety of uncertainty, and protect your relationship through the process.
The bottom line
Unexplained infertility is not a verdict. It's a gap in our current testing — a reflection of what medicine can and can't measure right now. For many couples, the cause eventually reveals itself through further investigation or during the IVF process itself. For others, conception happens naturally, sometimes after years of trying, sometimes during a break from treatment.
What matters most is that you don't accept "we don't know" as a full stop. Push for additional testing. Explore evidence-based treatments in a logical sequence. Protect your mental health. And remember that this diagnosis, frustrating as it is, doesn't define your body or your future.
You're not broken. You're navigating a system that hasn't caught up with the complexity of human reproduction. And there are still plenty of paths forward.
Frequently asked questions
▸Is unexplained infertility a real diagnosis or does it just mean my doctor stopped looking?
It's a bit of both. Clinically, it means no cause was found after standard testing — which covers ovulation, tubes, semen analysis, and the uterine cavity. But standard testing has limits. It doesn't check for silent endometriosis, sperm DNA fragmentation, immune factors, or chronic endometritis. Many couples labelled "unexplained" later discover a cause when they push for additional investigation.
▸Can I have endometriosis even with no symptoms?
Yes — this is called "silent endometriosis" and it's one of the most common hidden causes of unexplained infertility. Endometriosis can only be definitively diagnosed through laparoscopic surgery. Research suggests it may be present in 25–50% of unexplained cases. If you've had failed IUI or IVF cycles, it's worth discussing a diagnostic laparoscopy with your specialist.
▸Should I go straight to IVF or try IUI first?
For most couples under 37, IUI with ovarian stimulation is a reasonable first step. Per-cycle success rates are around 10–15%, and most specialists recommend three cycles before escalating. However, if you're over 37, have been trying for more than two years, or have had failed IUI cycles, moving to IVF sooner may be more time-efficient. IVF also acts as a diagnostic tool — it reveals issues that no other test can detect.
▸What tests should I ask for beyond the standard workup?
Beyond the standard fertility tests, consider asking about: sperm DNA fragmentation testing (not covered by standard semen analysis), diagnostic laparoscopy for silent endometriosis, endometrial biopsy (EMMA/ALICE test) for chronic endometritis, ReceptivaDx or BCL6 testing as a less invasive alternative to surgery for endo markers, and vitamin D levels — deficiency is common and linked to implantation failure.
▸Has anyone gotten pregnant naturally after an unexplained infertility diagnosis?
Yes. Research shows that up to 43% of people with unexplained infertility eventually conceive without treatment. Spontaneous conception rates of 13–15% have been documented in the first year after diagnosis, rising to around 35% over three years. However, the probability decreases over time, which is why active intervention is recommended — especially for women over 35.
▸Does stress cause unexplained infertility?
The relationship between stress and fertility is complex. Severe chronic stress can disrupt ovulation through the hypothalamic-pituitary axis, but everyday stress — work pressure, TTC anxiety — is unlikely to be the sole cause of infertility. What's clearer is that infertility itself causes significant psychological distress (up to 40% of women with infertility have clinical depression or anxiety), and that distress can create a vicious cycle. Getting mental health support is important regardless of whether stress "caused" the problem.
▸How long should we keep trying naturally before seeking treatment?
If you're under 35 and have been trying for over 12 months, or over 35 and trying for 6 months, it's time to seek a fertility referral. After an unexplained diagnosis, NICE recommends two years of expectant management before IVF — but many specialists feel this is too long, particularly for women approaching 35 or older. A reasonable approach: try for 6 months with lifestyle optimisation, then move to active treatment if not pregnant. Discuss your specific timeline with a fertility specialist.
References
- Raperport, S. et al. (2026). Unexplained Infertility: An Update. The Obstetrician & Gynaecologist. doi:10.1111/tog.70037
- StatPearls (2026). Female Infertility. NCBI Bookshelf. NBK556033
- ASRM Practice Committee (2020). Evidence-based treatments for couples with unexplained infertility: a guideline. Fertility and Sterility, 113(2), 307–321.
- PMC (2023). Should IUI replace IVF as first-line treatment for unexplained infertility? BMC Women's Health, 23, 595. doi:10.1186/s12905-023-02717-1
- Brandes, M. et al. (2011). Unexplained infertility: overall ongoing pregnancy rate and mode of conception. Human Reproduction, 26(2), 360–368. PMID: 21163857
- Brosens, I. et al. (2013). Endometriosis and implantation: the missing pieces. Reproductive BioMedicine Online, 27(5), 463–468.
- Karayiannis, D. et al. (2018). Association between adherence to the Mediterranean diet and semen quality parameters in male partners of couples attempting fertility. Human Reproduction, 33(1), 215–222.
- Aitken, R.J. & Curry, B.T. (2011). Redox regulation of human sperm function: from the physiological control of sperm capacitation to the etiology of infertility and DNA damage in the germ line. Antioxidants & Redox Signaling, 14(3), 367–381.
⚕️ Medical Disclaimer
The information in this article is for educational purposes only and is not a substitute for professional medical advice. Always consult your GP, fertility specialist, or healthcare provider before making decisions about your fertility treatment. If you're experiencing symptoms of infertility, please seek medical guidance.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











