The Luteal Phase Explained: Why It Matters for Getting Pregnant
A nutritionist's guide to the luteal phase, progesterone, and what actually matters for implantation


The half of your cycle nobody talks about
Most fertility advice focuses on ovulation. Track your LH surge, time intercourse, wait and hope. But ovulation is only half the story. What happens after the egg is released — during the luteal phase — is just as important for getting pregnant, and it's the part most women know the least about.
I didn't fully appreciate this until I was deep into my own fertility journey. I was so focused on whether I was ovulating (I was) that I barely thought about what came next. But the luteal phase is where implantation either happens or doesn't. It's where progesterone either supports a pregnancy or fails to. And when things go wrong in this phase, they're often fixable — if you know what to look for.
What happens during the luteal phase
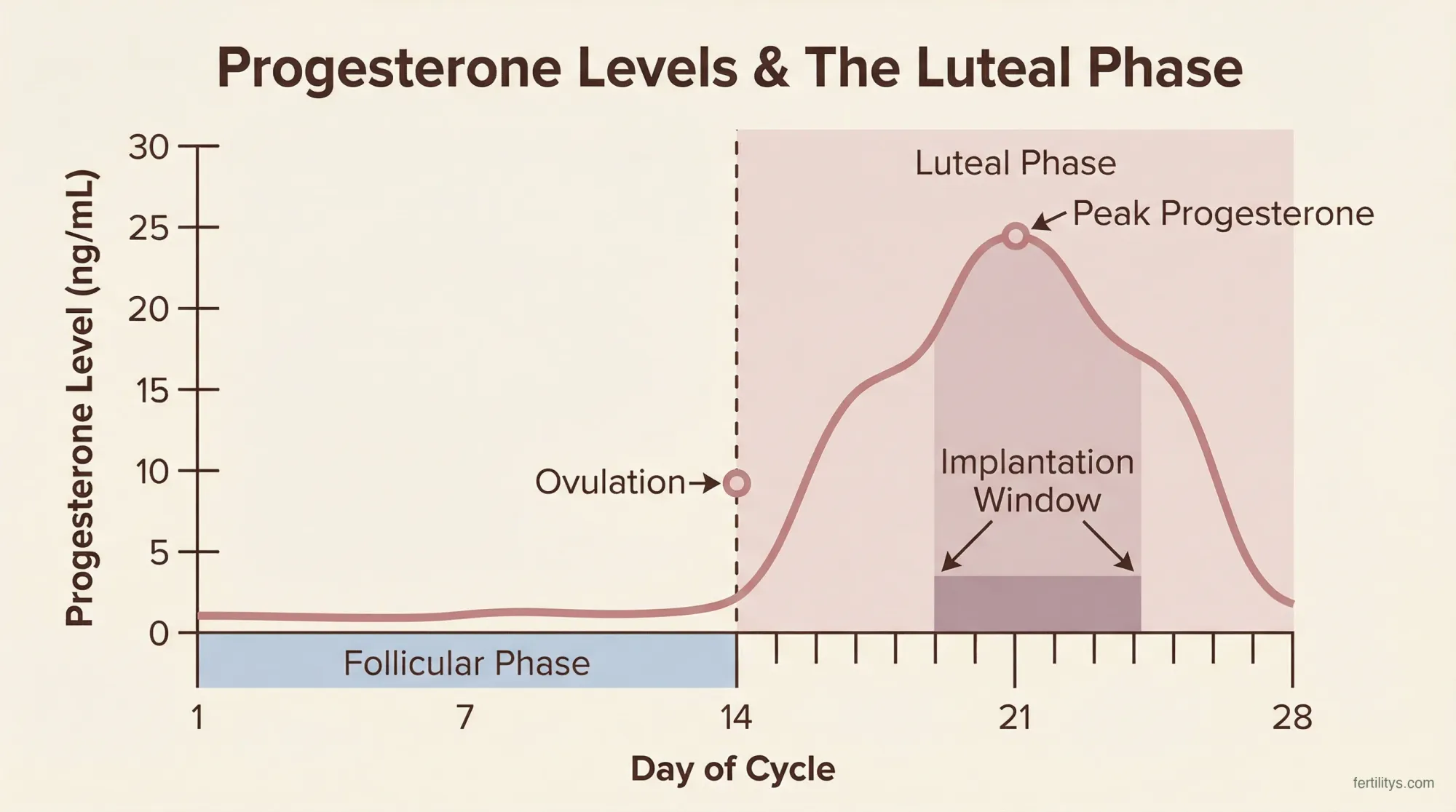
The moment you ovulate, the empty follicle on your ovary transforms into a temporary structure called the corpus luteum. This small, yellow-tinged cluster of cells has one primary job: producing progesterone.
Progesterone does three things that matter for conception:
- Thickens and stabilises your uterine lining — transforming it from a proliferative state into a secretory one that can support implantation
- Creates the implantation window — a brief period (roughly 6–10 days after ovulation) when the endometrium is receptive to an embryo
- Suppresses uterine contractions — keeping the lining stable so an embryo can attach and burrow in
Progesterone levels rise steadily after ovulation, typically peaking around 6–8 days post-ovulation at somewhere between 10 and 25 ng/mL (Mesen and Young, 2015). If no pregnancy occurs, the corpus luteum breaks down after about 12–14 days, progesterone drops, and your period starts. If an embryo does implant, it releases hCG, which signals the corpus luteum to keep producing progesterone until the placenta takes over around weeks 8–10.
This entire sequence depends on adequate progesterone. Without it, the lining can't sustain itself — and a fertilised egg either can't implant or can't stay implanted.
How long should the luteal phase be?
A normal luteal phase lasts between 10 and 16 days, with 12–14 days being most common. Unlike the follicular phase (which can vary wildly from cycle to cycle), the luteal phase is remarkably consistent for each individual woman — usually within a day or two each month.
This matters because consistency is what allows your body to prepare the lining at the right pace. If your luteal phase is consistently under 10 days, there may not be enough time for an embryo to implant before progesterone drops and the lining starts to shed. This is sometimes called a short luteal phase, and it's one of the more underdiagnosed fertility issues.
| Luteal Phase Length | What It Means for Fertility |
|---|---|
| Under 10 days | Potentially too short for implantation. Worth investigating with your doctor, especially if you've been trying for 6+ months. |
| 10–11 days | On the shorter side but usually adequate. Monitor and discuss with your GP if conception isn't happening. |
| 12–14 days | The sweet spot. Most pregnancies occur with luteal phases in this range. |
| 15–16 days | Longer than average but normal. If consistently over 16 days, take a pregnancy test — a persistently long luteal phase can be an early sign. |
One thing I tell my clients: don't obsess over a single cycle. Track your luteal phase over 3–4 months to see your personal pattern. One short cycle doesn't mean there's a problem. A consistent pattern of 8–9 day luteal phases is something to bring to your doctor.
How to calculate your luteal phase length
Count from the day after ovulation (confirmed by temperature rise, LH test, or cervical mucus shift) to the day before your next period starts. If you ovulated on day 14 and your period arrived on day 28, your luteal phase was 13 days.
The tricky part is confirming exactly when you ovulated. OPK strips detect the LH surge that precedes ovulation by 24–36 hours, so the actual ovulation day is usually the day after a positive OPK. Basal body temperature (BBT) confirms ovulation after it happens — the sustained temperature shift marks the start of the luteal phase. For the most accurate picture, I recommend using both methods together. Our ovulation calculator can help with timing.
Progesterone: the hormone that makes or breaks implantation
If the luteal phase had a main character, it would be progesterone. This hormone doesn't just thicken the uterine lining — it fundamentally changes its structure to make implantation possible.
After ovulation, progesterone triggers the endometrial glands to start secreting nutrients (glycogen, lipids, and proteins) that will feed an embryo in its earliest days, before the placenta develops. It also modifies the immune environment of the uterus, creating a kind of local tolerance so the body doesn't reject what is, immunologically speaking, a foreign entity (Mesen and Young, 2015).
The American Society for Reproductive Medicine (ASRM) considers a mid-luteal progesterone level above 3 ng/mL as confirmation that ovulation occurred (ASRM, 2021). But "ovulation happened" and "progesterone is adequate for pregnancy" are two different things. Most fertility specialists want to see mid-luteal progesterone at 10 ng/mL or above for the best chance at successful implantation.
| Mid-Luteal Progesterone (ng/mL) | Interpretation |
|---|---|
| Under 3 | Ovulation likely didn't occur (anovulatory cycle) |
| 3–10 | Ovulation confirmed, but progesterone may be suboptimal for implantation |
| 10–25 | Normal luteal phase range — adequate for implantation |
| Over 25 | High-normal. Can indicate strong ovulation or early pregnancy |
Here's what complicates things: progesterone is secreted in pulses, not as a steady stream. A single blood draw at 2pm might show 8 ng/mL, while the same woman tested at 9am might show 14 ng/mL. This is why the ASRM cautions against diagnosing luteal phase defect based on a single progesterone level. If your doctor is concerned about low progesterone, serial testing (multiple draws across the luteal phase) gives a much more accurate picture.
Luteal phase defect: when the system breaks down
A luteal phase defect (LPD) happens when the corpus luteum doesn't produce enough progesterone, or the uterine lining doesn't respond adequately to the progesterone that's there. The result is an endometrium that can't sustain implantation — either because the lining is too thin, because it starts shedding too early, or because the implantation window doesn't open properly.
LPD is genuinely controversial in reproductive medicine. The ASRM's 2021 committee opinion states that while the condition is "a concept that has existed in the medical literature for decades," there's no reliable test to diagnose it and no clear evidence that treating it improves pregnancy rates in natural cycles (ASRM, 2021). A 2024 review in Reproductive Sciences echoed this, noting that "the perceived relationship between LPD and recurrent pregnancy loss is challenged by conflicting data" (Bukulmez, 2024).
That said, plenty of fertility specialists do take it seriously, particularly when a woman has:
- Consistently short luteal phases (under 10 days)
- Recurrent early miscarriages
- Low mid-luteal progesterone on serial testing
- Premenstrual spotting starting several days before the period
The honest answer? We don't have perfect diagnostic criteria for LPD, and that's frustrating. But if your luteal phase is consistently short and you're not conceiving, it's absolutely worth investigating — even if the diagnosis itself is debated.
What causes luteal phase problems
Several underlying factors can disrupt the luteal phase:
Thyroid disorders — Both hypothyroidism and hyperthyroidism can shorten the luteal phase or reduce progesterone production. A full thyroid panel (TSH, free T3, free T4, thyroid antibodies) is a reasonable starting point for any woman with a suspected luteal phase issue.
High prolactin — Elevated prolactin interferes with GnRH pulsatility, which disrupts the LH support that the corpus luteum needs to produce progesterone. This is treatable with medication.
Excessive exercise or low body weight — The hypothalamic-pituitary-ovarian axis is sensitive to energy availability. Intense training or very low body fat can lead to subtle ovulatory dysfunction where ovulation happens but the luteal phase is compromised.
PCOS — While PCOS is more commonly associated with anovulation, women with PCOS who do ovulate may have suboptimal luteal phase quality due to abnormal follicular development.
Stress — Chronic stress raises cortisol, which competes with progesterone for receptors and can suppress the hypothalamic signals that drive luteal function. I see this a lot in my clients — the irony of fertility stress undermining the very hormones needed for conception isn't lost on anyone going through it.
Age — Luteal phase quality can decline with age, partly because follicle quality affects corpus luteum function. A poorer-quality follicle tends to produce a poorer-quality corpus luteum.
How to support your luteal phase naturally
Before I get into this: if you suspect a genuine luteal phase defect, work with your doctor. Natural approaches can help optimise a functional luteal phase, but they're not a replacement for medical treatment when there's an underlying condition like thyroid disease or hyperprolactinaemia.
That said, there's plenty you can do to give your luteal phase the best chance:
Vitamin B6 — This is probably the most commonly recommended supplement for luteal phase support, and there's some basis for it. B6 is involved in progesterone receptor function, and a small body of evidence suggests it may help lengthen a short luteal phase. I typically suggest 50–100mg daily (as P5P, the active form) during the luteal phase, though the evidence is limited to small studies.
Vitamin C — A 2003 study in Fertility and Sterility found that women taking 750mg of vitamin C daily had significantly higher progesterone levels and higher pregnancy rates compared to a control group (Henmi et al., 2003). It's a small study, but the mechanism (antioxidant protection of the corpus luteum) makes biological sense.
Vitex (chasteberry) — Vitex acts on the pituitary to modulate prolactin levels, which can indirectly support progesterone production. It's the most-studied herbal remedy for luteal phase issues, with several trials showing improvements in cycle regularity and progesterone levels. But it takes 3–6 months to show effects, and it's not appropriate for everyone — particularly not alongside fertility medications.
Adequate fat intake — Cholesterol is the building block of all sex hormones, including progesterone. Very low-fat diets can genuinely compromise hormone production. I recommend at least 60–80g of healthy fats daily from sources like avocado, olive oil, nuts, seeds, and oily fish. This was a big part of my own dietary shift — switching to a Mediterranean-style diet that didn't shy away from fats.
Manage stress actively — Not the "just relax and it'll happen" kind of advice (which is useless and insulting). I mean structured approaches: regular yoga, breathing exercises, acupuncture, therapy, or whatever genuinely brings your cortisol down. During my own fertility journey, I replaced HIIT with gentle movement and added fertility acupuncture — both made a noticeable difference to how my body handled the two-week wait.
Prioritise sleep — Progesterone production is partly regulated by circadian rhythms. Disrupted sleep patterns can reduce the pulsatile secretion of LH that the corpus luteum depends on. Aim for 7–9 hours, consistent bed and wake times, and limited blue light exposure after 9pm.
Medical treatment for luteal phase issues
If natural approaches aren't enough — or if there's a clear medical cause — your doctor may suggest one of several treatments:
Progesterone supplementation — The most direct approach. Vaginal progesterone pessaries (200–400mg daily) or oral micronised progesterone (Utrogestan) started after ovulation can support the luteal phase through the implantation window. A meta-analysis of randomised trials found that luteal progesterone supplementation significantly improved fertility outcomes compared to no treatment (Daya and Gunby, 2004). This is standard practice in IVF cycles but increasingly used in natural and medicated cycles too.
hCG injections — Injection of hCG in the luteal phase mimics the natural hCG signal from an implanting embryo, stimulating the corpus luteum to continue producing progesterone. The same meta-analysis found hCG equally effective to progesterone supplementation.
Clomiphene citrate or letrozole — These ovulation-stimulating medications can improve follicular development, which in turn produces a better-quality corpus luteum with stronger progesterone output. If the root cause of your luteal phase issue is suboptimal ovulation, this addresses the upstream problem rather than just supplementing progesterone downstream.
Thyroid medication — If thyroid dysfunction is driving the issue, treating it often resolves the luteal phase problem entirely. Even subclinical hypothyroidism (TSH between 2.5 and 4.5 mIU/L) can affect the luteal phase, and many fertility specialists now aim for TSH under 2.5 in women trying to conceive.
Tracking your luteal phase: what to monitor
If you're trying to conceive, tracking your luteal phase gives you genuinely useful data — both for yourself and for any fertility specialist you see later. Here's what to record:
Basal body temperature (BBT) — Your temperature rises 0.2–0.5°C after ovulation due to progesterone's thermogenic effect and stays elevated throughout the luteal phase. If it drops before day 10 post-ovulation, that's a potential red flag. A sustained rise past day 16 is an early pregnancy sign. Our luteal phase symptoms guide covers what to expect.
Cervical mucus changes — After ovulation, progesterone shifts cervical mucus from the stretchy, egg-white consistency of the fertile window to thicker, stickier, or drier discharge. Monitoring this pattern helps confirm the luteal transition. More detail in our luteal phase discharge article.
Cycle length and consistency — If your total cycle length varies significantly month to month, it's usually the follicular phase that's varying, not the luteal phase. But if you notice your period coming earlier and earlier, it's worth checking whether your luteal phase is shortening.
Spotting patterns — Premenstrual spotting starting 3+ days before your full period can indicate declining progesterone. Occasional spotting is normal, but a consistent pattern is worth mentioning to your doctor.
Day 21 (or 7 DPO) progesterone test — This blood test, timed to your mid-luteal phase (not necessarily day 21 — that only works if you ovulate on day 14), is the most commonly used clinical marker for luteal function. Ask your GP for this if you've been trying for 6+ months.
When to see your doctor
Book an appointment if you notice any of these patterns:
- Your luteal phase is consistently under 10 days (tracked over 3+ cycles)
- You're experiencing premenstrual spotting that starts 4+ days before your period, every cycle
- You've had two or more early miscarriages (before 8 weeks)
- You've been tracking ovulation and timing intercourse for 6+ months (under 35) or 3+ months (over 35) without conceiving
- You have other symptoms suggesting a hormonal issue — fatigue, hair changes, weight changes, persistent mood changes in the second half of your cycle
In the UK, your GP can order a day 21 progesterone test and thyroid panel. If these come back suboptimal, they may refer you to a fertility clinic for further investigation. In the US, you can often self-refer to a reproductive endocrinologist.
The bottom line
The luteal phase is the quiet half of your cycle, but it's where conception actually becomes pregnancy. Progesterone rises, your lining transforms, and if a fertilised egg arrives, it either finds a welcoming environment — or it doesn't.
If you're tracking ovulation but not thinking about what happens after, you're missing half the picture. A luteal phase that's too short, progesterone that's too low, or an underlying condition that's disrupting the process can all be addressed — but only if you know to look.
Track your cycles, know your luteal phase length, and don't hesitate to ask your doctor about progesterone testing if something feels off. Your body is giving you information. Pay attention to it.
▸Can you get pregnant with a short luteal phase?
Yes, but it's harder. A luteal phase under 10 days may not give a fertilised egg enough time to implant before progesterone drops and the lining starts to shed. Treatment with progesterone supplementation or ovulation-stimulating medication can help lengthen a short luteal phase and improve your chances.
▸What progesterone level do you need to get pregnant?
A mid-luteal progesterone level of 10 ng/mL or above is generally considered optimal for implantation. Levels above 3 ng/mL confirm ovulation occurred, but anything between 3 and 10 may be suboptimal for sustaining a pregnancy. Your doctor can test this with a blood draw timed 7 days after ovulation.
▸Does a luteal phase defect cause miscarriage?
The relationship between luteal phase defect and miscarriage is debated among specialists. The ASRM states there's no reliable test to diagnose LPD or clear evidence linking it to pregnancy loss. However, many fertility doctors do treat suspected LPD with progesterone supplementation, particularly in women with recurrent early miscarriages. If you've experienced recurrent losses, ask your doctor about progesterone testing.
▸Is it normal for luteal phase length to change?
Small variations of 1–2 days between cycles are completely normal. The luteal phase is actually the most consistent part of the menstrual cycle for most women. If you notice a sudden change of 3+ days, or a progressive shortening over several months, it's worth investigating — particularly if you're trying to conceive.
▸Can stress shorten your luteal phase?
Yes. Chronic stress raises cortisol, which can suppress the hypothalamic-pituitary signals that drive progesterone production. This can shorten the luteal phase or reduce progesterone levels enough to affect implantation. Structured stress management — yoga, meditation, therapy, acupuncture — may help, though the evidence is mainly observational.
▸When should I get my progesterone tested?
The standard timing is 7 days after ovulation (often called a "day 21 test," but only if you ovulate on day 14). If you ovulate later, adjust accordingly — the test needs to catch your mid-luteal peak. Ask your GP for this test if you've been trying to conceive for 6+ months, or sooner if you've had recurrent miscarriages or suspect a short luteal phase.
References
- Mesen, T.B. and Young, S.L. (2015). Progesterone and the Luteal Phase: A Requisite to Reproduction. Obstetrics and Gynecology Clinics of North America, 42(1), pp.135–151. doi:10.1016/j.ogc.2014.10.003
- ASRM Practice Committee (2021). Diagnosis and Treatment of Luteal Phase Deficiency: A Committee Opinion. Fertility and Sterility, 115(6), pp.1416–1423. Link
- Bukulmez, O. (2024). Luteal Phase Defects and Progesterone Supplementation. Reproductive Sciences. PMID:38377455
- Daya, S. and Gunby, J.L. (2004). Luteal phase support in assisted reproduction cycles. Cochrane Database of Systematic Reviews. PMID:12202415
- Henmi, H. et al. (2003). Effects of ascorbic acid supplementation on serum progesterone levels in patients with a luteal phase defect. Fertility and Sterility, 80(2), pp.459–461.
- NHS (2024). Periods and Fertility in the Menstrual Cycle. nhs.uk
- ACOG (2021). Bleeding During Pregnancy. FAQ038. acog.org
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your health routine or starting any new supplement. Fertilitys does not provide medical diagnoses or treatment recommendations.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.