AMH Levels by Age: What's Normal and What Your Numbers Mean
A fertility nutritionist's complete guide to AMH levels by age — with a chart based on 22,920 women, what your numbers actually mean, and why AMH isn't the whole story.


When I got my AMH result back at 32, it was 3 pmol/L. I didn't even know what AMH was six months earlier, and suddenly this single number felt like it defined my entire future. I remember googling "normal AMH for 32" in the clinic car park, scrolling through confusing charts with different units, and feeling more lost than before the test.
That experience is exactly why I wrote this article. AMH levels by age is one of the most searched fertility topics online — and one of the most poorly explained. Most charts give you a number without any context about what it actually means for your chances of getting pregnant.
So here's what I wish someone had told me: your AMH level matters, but it's not a fertility sentence. Let me walk you through what the numbers actually mean, what's normal for your age, and — just as importantly — what AMH can't tell you.
What Is AMH and Why Does It Matter?
Anti-Müllerian hormone (AMH) is a protein produced by the granulosa cells surrounding your developing egg follicles. Think of it as a rough headcount of your remaining egg supply — what doctors call your ovarian reserve.
Unlike FSH or oestradiol, AMH stays relatively stable throughout your menstrual cycle, which means you can test it on any day. No fasting required, no specific cycle day to hit. It's a simple blood test that gives your doctor a snapshot of how many eggs you have left — though not how good those eggs are. That's a distinction I'll come back to, because it's one most people miss.
AMH is measured in either ng/mL or pmol/L depending on your country. The UK typically uses pmol/L, while the US and many other countries use ng/mL. To convert: 1 ng/mL = 7.14 pmol/L. I'll include both units throughout this article so you don't have to do the maths yourself.
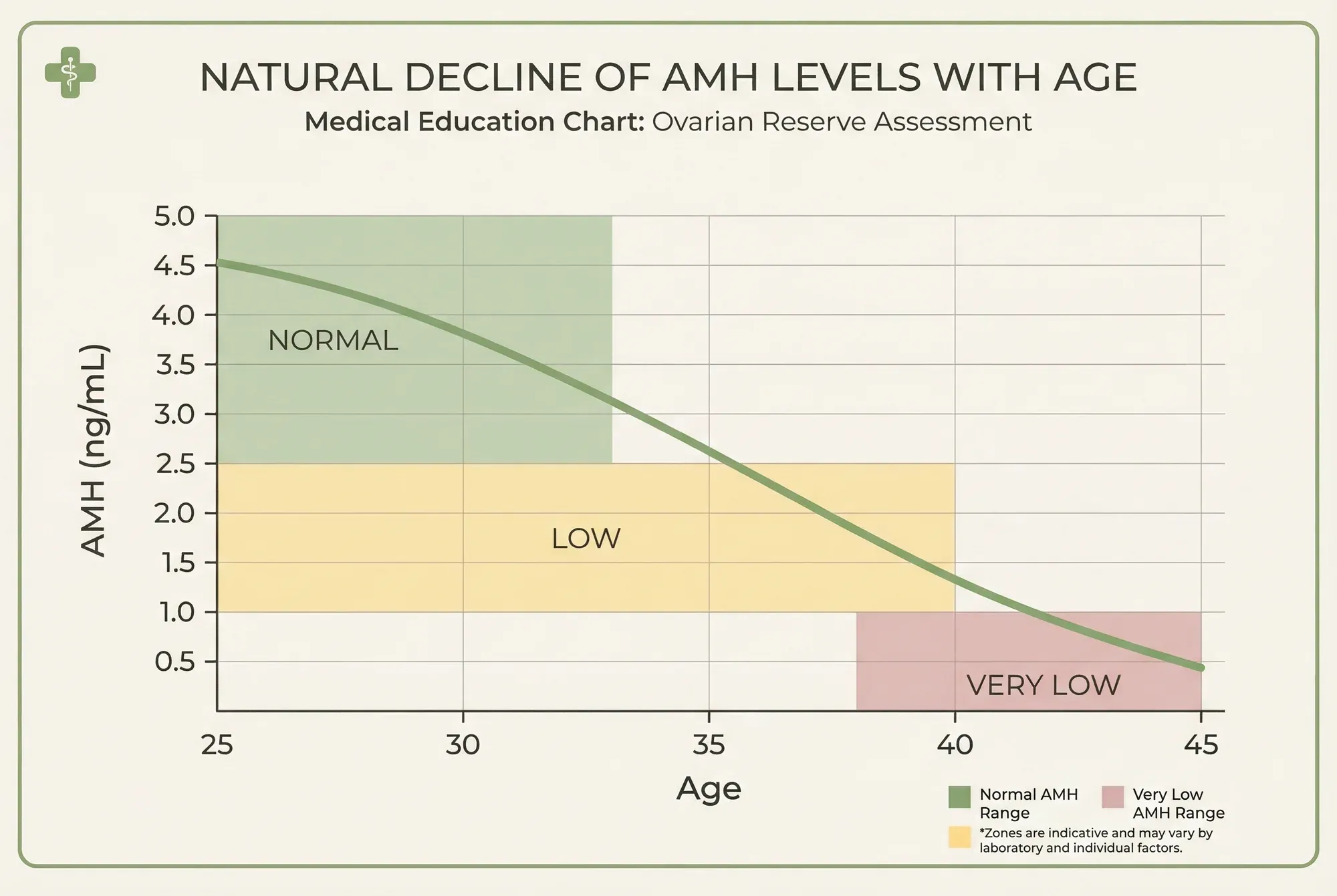
Normal AMH Levels by Age: The Complete Chart
This table is based on the largest recent AMH study — a 2025 analysis of 22,920 women aged 18 to 45 (Tukiendorf et al., Frontiers in Endocrinology). I've included the median (the middle value) along with the 25th and 75th percentiles, so you can see the normal range — not just a single number. I've also added the pmol/L conversion for each value.
| Age | Median AMH (ng/mL) | Median AMH (pmol/L) | 25th–75th Percentile (ng/mL) | % With Low AMH |
|---|---|---|---|---|
| 20 | 4.2 | 30.0 | 2.5 – 6.7 | 8.5% |
| 22 | 4.1 | 29.3 | 2.2 – 6.4 | 10.5% |
| 25 | 3.3 | 23.6 | 1.9 – 5.7 | 13.5% |
| 27 | 3.1 | 22.1 | 1.7 – 5.3 | 16.2% |
| 28 | 2.8 | 20.0 | 1.5 – 4.9 | 18.6% |
| 30 | 2.5 | 17.9 | 1.2 – 4.3 | 24.3% |
| 32 | 2.0 | 14.3 | 0.9 – 3.8 | 33.2% |
| 33 | 1.8 | 12.9 | 0.8 – 3.3 | 36.7% |
| 35 | 1.4 | 10.0 | 0.5 – 2.9 | 45.7% |
| 36 | 1.1 | 7.9 | 0.4 – 2.3 | 52.9% |
| 37 | 1.0 | 7.1 | 0.3 – 2.3 | 55.8% |
| 38 | 0.7 | 5.0 | 0.2 – 1.7 | 64.0% |
| 40 | 0.5 | 3.6 | 0.2 – 1.3 | 73.0% |
| 42 | 0.3 | 2.1 | 0.1 – 0.8 | 85.0% |
| 45 | 0.1 | 0.7 | 0.05 – 0.3 | 96.0% |
Source: Tukiendorf et al. (2025), Frontiers in Endocrinology. "Low AMH" defined as <1.2 ng/mL (<8.6 pmol/L) per the Poseidon Classification. N = 22,920.
The chart below shows how my own AMH levels compared to these reference ranges — and how they changed after I implemented my nutritional protocol.
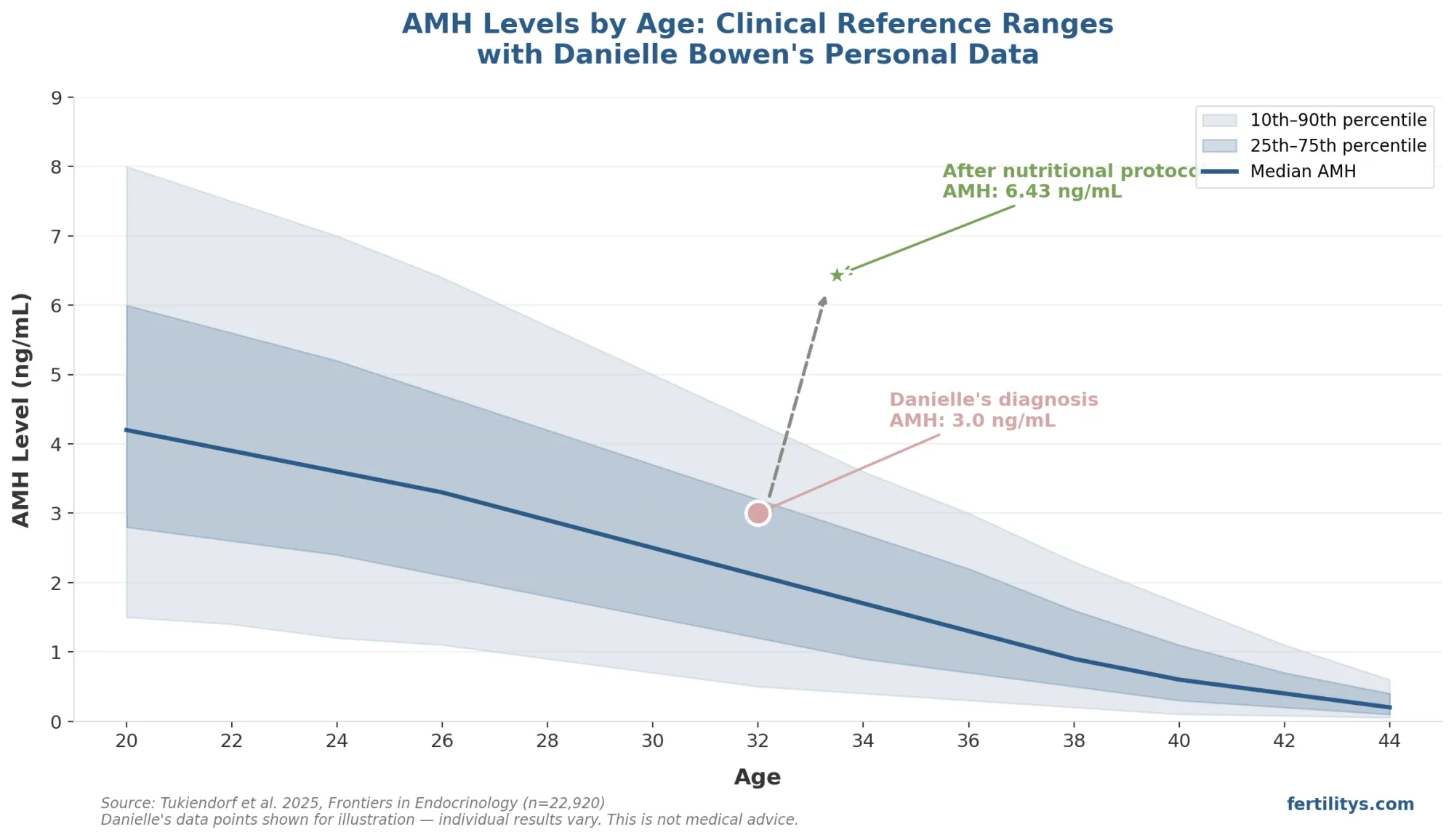
Danielle's AMH levels (3.0 → 6.43 ng/mL) plotted against clinical reference ranges from Tukiendorf et al. 2025 (n=22,920). Individual results vary.
A few things jump out from this data. The decline isn't gradual and steady — it accelerates sharply after 35. By 36, more than half of women have AMH below the clinical threshold for diminished ovarian reserve. And even at younger ages, the range is enormous: a 25-year-old could have an AMH anywhere from 1.9 to 5.7 ng/mL and still be perfectly normal.
My own AMH at 32 was 3 pmol/L — that's about 0.42 ng/mL. According to this chart, the median for a 32-year-old is 2.0 ng/mL. Mine was less than a quarter of that. I was in the bottom few percent for my age. So I understand the panic when you see a number that's far from the median. But here's what the chart can't show you: I went on to conceive naturally.
How to Read Your AMH Result
Most fertility clinics categorise AMH results into broad ranges. These cutoffs vary slightly between clinics and countries, but here's the general framework used across the UK and US:
| Category | ng/mL | pmol/L | What It Suggests |
|---|---|---|---|
| High | > 5.0 | > 35.7 | Large egg reserve; may indicate PCOS |
| Normal | 1.5 – 5.0 | 10.7 – 35.7 | Good ovarian reserve for age |
| Low–Normal | 1.0 – 1.5 | 7.1 – 10.7 | Below average; fertility still possible |
| Low | 0.5 – 1.0 | 3.6 – 7.1 | Diminished reserve; consider timeline |
| Very Low | < 0.5 | < 3.6 | Significantly reduced reserve |
But — and I really want to stress this — these categories need to be read alongside your age. An AMH of 1.5 ng/mL at 28 is low for your age group and worth investigating. The same AMH at 40 is actually above the median and perfectly reasonable.
Context changes everything. And units matter too. I've seen women in complete distress because they thought their AMH of 15 was catastrophically low — when it was actually 15 pmol/L, which converts to 2.1 ng/mL, a perfectly healthy level. Always check which units your clinic uses.
AMH Levels by Age With PCOS
If you have PCOS, your AMH picture looks quite different. Women with polycystic ovary syndrome typically have AMH levels 2-4 times higher than women without PCOS, because the large number of small follicles on polycystic ovaries produce more of the hormone (Iliodromiti et al., 2013).
Research suggests that an AMH above 3.8–5.0 ng/mL (27–36 pmol/L) may be a marker for PCOS, though there's no universally agreed cutoff yet (Dewailly et al., 2014). The 2023 international PCOS guidelines from the Teede group now recognise AMH as a potential diagnostic alternative to ultrasound — particularly useful for younger women and adolescents where transvaginal scanning isn't appropriate.
Here's what's interesting about PCOS and AMH over time: a 2012 study in Fertility and Sterility found that women with PCOS actually experience a more rapid rate of AMH decline than women without PCOS — even though they start higher. Their average AMH was 6.1 ng/mL compared to 1.8 ng/mL in controls. So while the starting point is elevated, the trajectory is steeper.
I work with a lot of PCOS clients, and the first thing I tell them is: a high AMH doesn't automatically mean you're more fertile. It means you have more follicles, but PCOS often comes with ovulation problems, and ovulation is what actually gets you pregnant — not follicle count.
What Your AMH Level Can and Can't Tell You
This is the section I wish every clinic would pin to their wall. AMH is genuinely useful — but it's frequently over-interpreted, and the anxiety that creates is real.
What AMH Can Tell You
AMH gives a reliable estimate of your ovarian reserve — the approximate number of eggs you have remaining. This matters for:
- IVF planning — AMH predicts how well your ovaries will respond to stimulation drugs. Higher AMH typically means more eggs retrieved (Broer et al., 2013).
- Egg freezing decisions — knowing your reserve helps you plan timing. A lower AMH at 30 might push you to freeze sooner rather than later.
- Understanding your timeline — if your AMH is declining faster than expected for your age, you and your doctor can make more informed decisions about when to try.
What AMH Cannot Tell You
And here's where most people get it wrong:
- AMH does not measure egg quality. A woman with an AMH of 0.5 ng/mL can have perfectly healthy eggs. A woman with an AMH of 8 ng/mL can have poor-quality eggs. The 2017 JAMA study by Steiner et al. — which followed 750 women trying to conceive naturally — found no significant difference in pregnancy rates between women with low AMH and women with normal AMH. Let that sink in.
- AMH is not a fertility test. It doesn't tell you whether you can get pregnant. It tells you approximately how many eggs are left. Those are very different questions.
- AMH doesn't account for your partner's fertility. Half of infertility cases involve male factor. Your AMH could be textbook-perfect and still not be the variable that matters.
When the clinic told me my AMH was 3 pmol/L, I heard "you can't have children." That's not what the number said. It said I had fewer eggs than expected. I still had eggs. And one of those eggs became my son.
What Causes AMH to Be Low for Your Age?
Some women have AMH levels well below the median for their age group. Before you spiral (I've been there), it's worth understanding the possible reasons:
- Natural variation — some women simply start with a smaller egg pool. It's genetic, like height or eye colour. The 2025 nomogram shows 13.5% of 25-year-olds already have AMH below 1.2 ng/mL. That's roughly 1 in 7.
- Endometriosis — the same nomogram study found women from the endometriosis clinic had significantly lower AMH (median 1.6 ng/mL) compared to 2.0 ng/mL in other departments. Ovarian endometriomas can damage follicles and reduce reserve.
- Previous ovarian surgery — removal of ovarian cysts, especially endometriomas, can reduce egg supply. Each surgery carries a risk of losing healthy tissue alongside the cyst.
- Smoking — smoking accelerates follicle loss. Studies consistently show that smokers reach menopause 1-4 years earlier than non-smokers (Freour et al., 2008).
- Autoimmune conditions — conditions like thyroid disease or premature ovarian insufficiency (POI) can cause faster-than-expected AMH decline.
- Chemotherapy or radiation — cancer treatments are directly toxic to ovarian follicles. If you're facing treatment, discuss fertility preservation before starting.
For me, there was no clear cause. No endometriosis, no surgery, no smoking. Just naturally lower than expected. It happens — and it doesn't mean nothing can be done.
Normal AMH for Age 35: A Closer Look
I'm giving 35 its own section because it's the age where most women start paying attention — and where the data gets particularly interesting.
According to the 2025 nomogram (22,920 women), the median AMH at 35 is 1.4 ng/mL (10.0 pmol/L). The normal range spans from 0.5 to 2.9 ng/mL (3.6–20.7 pmol/L). Nearly half (45.7%) of 35-year-olds already meet the clinical definition of diminished ovarian reserve.
That statistic isn't meant to frighten you — it's meant to recalibrate expectations. "Diminished ovarian reserve" sounds terrifying, but all it means clinically is that your AMH is below 1.2 ng/mL. Millions of women with AMH below that threshold conceive every year. The Steiner 2017 JAMA study specifically tested this: women aged 30–44 with low AMH (<0.7 ng/mL) had virtually the same 12-month conception rate as women with normal AMH when trying naturally.
If you're 35 with an AMH of 1.0 ng/mL, you're below the median but within the normal range. The most useful thing you can do isn't panic — it's optimise. Start prepping your body now, support your egg quality (because that's what actually determines pregnancy success, not quantity), and consider your timeline honestly.
⏳ Start Earlier Than You Think
I tell every client the same thing: give yourself at least 12 months of preparation before trying to conceive. Not the 3 months you'll see everywhere online — a full year. Egg development takes around 90 days from recruitment to ovulation, and the nutritional and lifestyle changes that support egg quality need time to take effect. The earlier you start, the more cycles you influence. This is especially true if your AMH is below the median for your age.
Can You Improve Your AMH Level?
This is the million-pound question, and I want to be honest with you: the evidence is mixed, and you need to be wary of anyone promising to "fix" your AMH.
AMH reflects your remaining follicle pool. You can't create new eggs — you were born with all of them. But what the research does show is that certain interventions may support the follicles you still have and, in some cases, lead to modest AMH increases:
- DHEA supplementation — a 2018 systematic review in Reproductive BioMedicine Online found DHEA supplementation (75mg/day) increased AMH in women with diminished ovarian reserve (Xu et al., 2018). It's the supplement with the strongest evidence for AMH improvement — but always take it under medical supervision.
- Vitamin D — women with vitamin D deficiency consistently show lower AMH. Correcting a deficiency may reveal your "true" AMH rather than actually increasing it (Dennis et al., 2012).
- CoQ10 — primarily supports mitochondrial function and egg quality rather than AMH directly, but some studies show a secondary AMH increase (Ben-Meir et al., 2015).
- Lifestyle optimisation — reducing inflammation, improving sleep, cutting alcohol, going organic where possible. These won't double your AMH, but they create the best environment for the eggs you have.
My own AMH went from 3 pmol/L (about 0.42 ng/mL) to 6.43 pmol/L (about 0.9 ng/mL) over 12 months. Was it the supplements? The diet overhaul? The stress reduction? Honestly, I don't know which individual piece made the difference. What I do know is that the combination of everything — CoQ10, vitamin D, omega-3, Mediterranean diet, gentle exercise, better sleep — created a measurably better picture. And more importantly, I got pregnant naturally.
When to Get Your AMH Tested
You don't need to wait until you're struggling. I actually recommend AMH testing to any woman who wants fertility awareness — ideally in your late twenties or early thirties. Think of it as a baseline, like knowing your cholesterol. It doesn't predict the future, but it gives you information to plan with.
Specific situations where testing is particularly valuable:
- You're over 30 and considering delaying pregnancy
- You're thinking about egg freezing
- You have a family history of early menopause
- You have endometriosis or have had ovarian surgery
- You've been trying to conceive for 6+ months without success
- You have PCOS and want to understand your ovarian reserve beyond the follicle count

In the UK, you can get AMH tested through your GP (though not all surgeries offer it routinely), through a fertility clinic, or through at-home testing kits. In the US, most reproductive endocrinologists include AMH as standard in a fertility workup. Costs range from free (NHS referral) to £50–150 (private/at-home) to $100–300 (US out-of-pocket).

The Bottom Line
AMH levels decline with age — that's biology, not a diagnosis. By 35, nearly half of women have AMH below 1.2 ng/mL, and the decline accelerates sharply after 36. Your number matters as a planning tool, especially for IVF or egg freezing. But AMH doesn't measure egg quality, doesn't predict natural conception, and doesn't define your fertility.
I know this because I lived it. An AMH of 3 pmol/L at 32 — bottom of the chart — and a healthy baby boy at the end of it. The number mattered for my planning. It didn't determine my outcome.
If your AMH is lower than you expected, take a breath. Then take action. Optimise what you can control — nutrition, supplements, lifestyle, stress. Give yourself a proper timeline (12 months, not 3). And get the full picture: AMH alongside AFC, FSH, and your partner's fertility. One number doesn't tell your whole story.
▸What is a normal AMH level by age chart?
Normal AMH varies widely by age. Median values from a 2025 study of 22,920 women: age 25 = 3.3 ng/mL (23.6 pmol/L), age 30 = 2.5 ng/mL (17.9 pmol/L), age 35 = 1.4 ng/mL (10.0 pmol/L), age 40 = 0.5 ng/mL (3.6 pmol/L). The 25th to 75th percentile range at each age is wide — there's no single "normal" number.
▸What is a normal AMH for a 35-year-old?
The median AMH at 35 is 1.4 ng/mL (10.0 pmol/L), with a normal range of 0.5–2.9 ng/mL (3.6–20.7 pmol/L). Nearly 46% of 35-year-olds have AMH below 1.2 ng/mL, which is the clinical threshold for diminished ovarian reserve — so "low" at 35 is more common than most people realise.
▸Does AMH predict fertility?
Not directly. AMH estimates your egg quantity (ovarian reserve), not egg quality. A 2017 JAMA study of 750 women found no significant difference in natural conception rates between women with low AMH and normal AMH. AMH is most useful for predicting IVF response and planning your fertility timeline — not for predicting whether you can get pregnant.
▸What do AMH levels by age look like with PCOS?
Women with PCOS typically have AMH levels 2–4 times higher than women without PCOS. An AMH above 3.8–5.0 ng/mL (27–36 pmol/L) may suggest PCOS, though diagnostic cutoffs aren't standardised yet. Despite starting higher, women with PCOS experience a faster rate of AMH decline over time.
▸Can you increase AMH levels naturally?
You can't create new eggs, but certain supplements may support your remaining follicles. DHEA has the strongest evidence for AMH improvement in women with diminished ovarian reserve. Vitamin D correction, CoQ10, and lifestyle optimisation (Mediterranean diet, stress reduction, sleep) may also help. My own AMH roughly doubled over 12 months with a combined protocol.
▸What AMH level is too low to conceive?
There's no AMH level that makes natural conception impossible while you're still having periods. Women with very low AMH (<0.5 ng/mL) have fewer eggs remaining but can still conceive — the eggs just need to be good quality. Research shows that even with AMH below 0.7 ng/mL, 12-month conception rates are similar to women with normal AMH when trying naturally. The real concern with very low AMH is time: your window for action may be shorter.
Frequently Asked Questions
▸What is a normal AMH level by age chart?
Normal AMH varies widely by age. Median values from a 2025 study of 22,920 women: age 25 = 3.3 ng/mL (23.6 pmol/L), age 30 = 2.5 ng/mL (17.9 pmol/L), age 35 = 1.4 ng/mL (10.0 pmol/L), age 40 = 0.5 ng/mL (3.6 pmol/L). The 25th to 75th percentile range at each age is wide — there's no single "normal" number.
▸What is a normal AMH for a 35-year-old?
The median AMH at 35 is 1.4 ng/mL (10.0 pmol/L), with a normal range of 0.5–2.9 ng/mL (3.6–20.7 pmol/L). Nearly 46% of 35-year-olds have AMH below 1.2 ng/mL, which is the clinical threshold for diminished ovarian reserve — so "low" at 35 is more common than most people realise.
▸Does AMH predict fertility?
Not directly. AMH estimates your egg quantity (ovarian reserve), not egg quality. A 2017 JAMA study of 750 women found no significant difference in natural conception rates between women with low AMH and normal AMH. AMH is most useful for predicting IVF response and planning your fertility timeline — not for predicting whether you can get pregnant.
▸What do AMH levels by age look like with PCOS?
Women with PCOS typically have AMH levels 2–4 times higher than women without PCOS. An AMH above 3.8–5.0 ng/mL (27–36 pmol/L) may suggest PCOS, though diagnostic cutoffs aren't standardised yet. Despite starting higher, women with PCOS experience a faster rate of AMH decline over time.
▸Can you increase AMH levels naturally?
You can't create new eggs, but certain supplements may support your remaining follicles. DHEA has the strongest evidence for AMH improvement in women with diminished ovarian reserve. Vitamin D correction, CoQ10, and lifestyle optimisation (Mediterranean diet, stress reduction, sleep) may also help. My own AMH roughly doubled over 12 months with a combined protocol.
▸What AMH level is too low to conceive?
There's no AMH level that makes natural conception impossible while you're still having periods. Women with very low AMH (<0.5 ng/mL) have fewer eggs remaining but can still conceive — the eggs just need to be good quality. Research shows that even with AMH below 0.7 ng/mL, 12-month conception rates are similar to women with normal AMH when trying naturally. The real concern with very low AMH is time: your window for action may be shorter.
▸What is a good AMH level for my age?
AMH varies significantly by age. Generally: under 25 (3.0-7.0 ng/mL), 25-30 (2.5-6.0), 30-35 (1.5-4.0), 35-40 (0.7-3.5), over 40 (0.3-1.5). But these are averages — individual variation is huge, and AMH is just one piece of the fertility picture.
▸Does AMH predict how many eggs I have left?
AMH correlates with your antral follicle count and gives an indication of ovarian reserve. However, it doesn't predict egg quality, your ability to conceive naturally, or how long your fertility will last. It's a useful data point, not a crystal ball.
▸Can AMH levels change?
AMH levels naturally decline with age. Short-term fluctuations can occur due to vitamin D status, hormonal contraception, or illness. Some lifestyle changes may modestly influence AMH, but dramatic increases are uncommon.
You might also find helpful:
References
- Tukiendorf et al. (2025). Age-stratified anti-Müllerian hormone (AMH) nomogram: a comprehensive cohort study including 22,920 women. Frontiers in Endocrinology, 16. doi:10.3389/fendo.2025.1612194
- Steiner AZ et al. (2017). Association Between Biomarkers of Ovarian Reserve and Infertility Among Older Women of Reproductive Age. JAMA, 318(14):1367-1376. doi:10.1001/jama.2017.14588
- Broer SL et al. (2013). AMH: a review of its role in ovarian function and clinical significance. Human Reproduction Update, 19(2):172-183. doi:10.1093/humupd/dms055
- Iliodromiti S et al. (2013). Can anti-Müllerian hormone predict the diagnosis of polycystic ovary syndrome? Journal of Clinical Endocrinology & Metabolism, 98(8):3332-3340. doi:10.1210/jc.2013-1571
- Dewailly D et al. (2014). Diagnosis of polycystic ovary syndrome (PCOS): revisiting the threshold values of follicle count and serum AMH level. Human Reproduction, 29(2):213-220. doi:10.1093/humrep/det410
- Xu L et al. (2018). Effects of DHEA administration on AMH levels in women with diminished ovarian reserve: a systematic review and meta-analysis. Reproductive BioMedicine Online, 36(5):535-544. doi:10.1016/j.rbmo.2018.01.014
- Dennis NA et al. (2012). The level of serum anti-Müllerian hormone correlates with vitamin D status in men and women. Journal of Clinical Endocrinology & Metabolism, 97(7):2450-2455. doi:10.1210/jc.2012-1106
- Ben-Meir A et al. (2015). Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell, 14(5):887-895. doi:10.1111/acel.12368
- Freour T et al. (2008). Active smoking compromises IVF outcome and affects ovarian reserve. Reproductive BioMedicine Online, 16(1):96-102.
- Teede HJ et al. (2023). International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Journal of Clinical Endocrinology & Metabolism, 108(10):e1241-e1244. doi:10.1210/clinem/dgad463
Medical Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice. Always consult your healthcare provider before making decisions about fertility testing or treatment. Danielle Bowen is a registered nutritionist (RNutr), not a medical doctor.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











