Molar Pregnancy: What It Is, Symptoms, Treatment and Recovery
A molar pregnancy is a rare abnormal pregnancy where placental tissue grows abnormally. Here's what it means, how it's treated, and what comes next.


📌 Key Takeaways
- A molar pregnancy is a rare complication where abnormal tissue grows instead of a healthy embryo — it affects roughly 1 in 1,000 pregnancies.
- Two main types exist: complete molar pregnancies (no embryo forms) and partial molar pregnancies (abnormal embryo with extra chromosomes).
- Early warning signs include heavy vaginal bleeding, severe nausea, and unusually high hCG levels detected in blood tests.
- Treatment typically involves a procedure called dilation and curettage (D&C) to remove the abnormal tissue, followed by careful monitoring of hCG levels.
- Most people go on to have healthy pregnancies after a molar pregnancy — your doctor will usually advise waiting 6–12 months before trying again.
Getting told your pregnancy is "molar" is one of the most disorienting things that can happen. You thought you were pregnant — you had the test, maybe even the early scan — and now someone's using words you've never heard, telling you there's no baby, and mentioning things like hCG monitoring and chemotherapy. It's a lot to take in.
I've walked clients through this, and I want you to know: most molar pregnancies are treated successfully, and most women go on to have healthy pregnancies afterward. But you deserve to understand what's happening, what comes next, and what your body needs during recovery.
Let's walk through this together.
What Is a Molar Pregnancy?
A molar pregnancy (also called a hydatidiform mole) is a type of gestational trophoblastic disease — a condition where the cells that would normally become the placenta grow abnormally. Instead of forming the tissue that feeds a developing baby, these cells form clusters that resemble a bunch of grapes. There's no viable pregnancy, and no baby can develop.
I always make sure my clients hear this clearly: it's not your fault. A molar pregnancy is caused by a genetic error during fertilisation — something that happens at the cellular level and cannot be prevented by anything you did or didn't do.
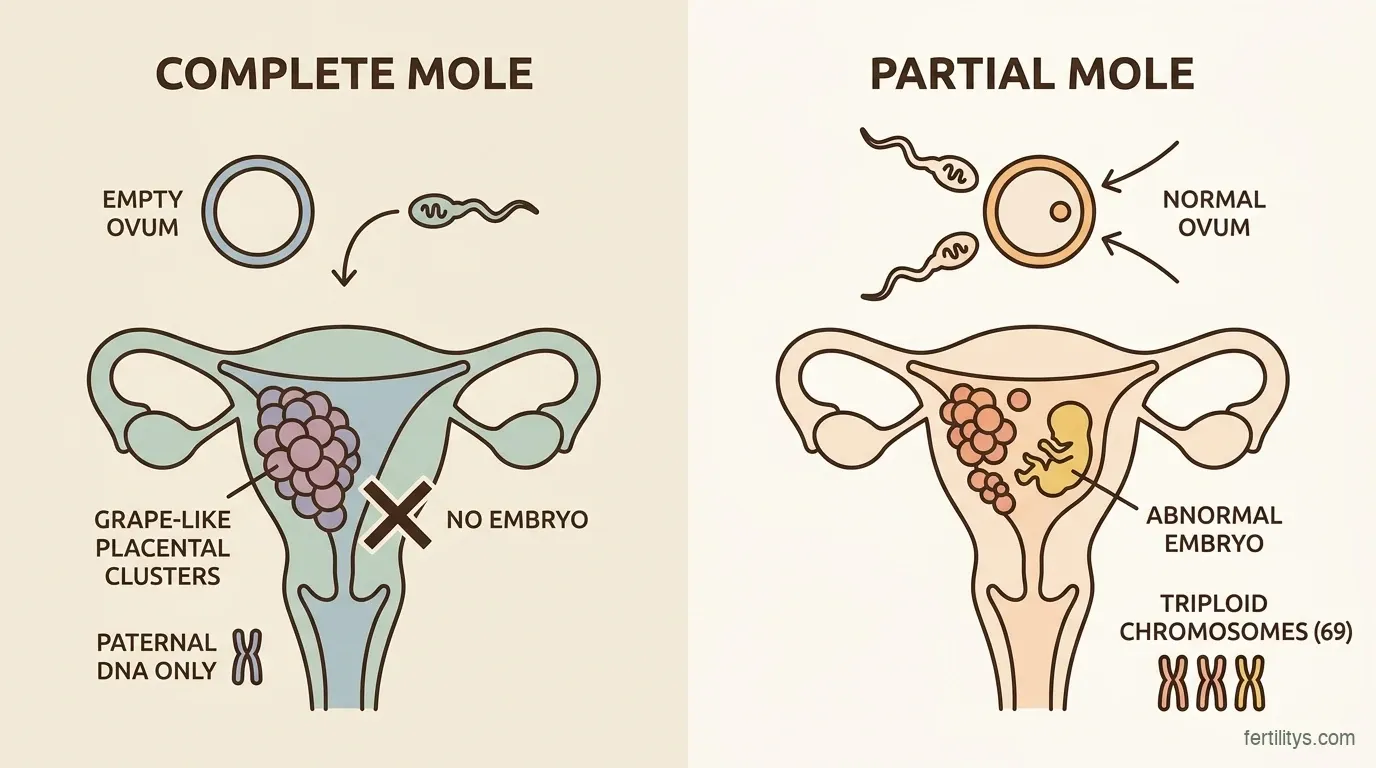
There are two types:
Complete molar pregnancy — An empty egg (one with no genetic material) is fertilised by one or two sperm. The result is only paternal DNA. No embryo forms at all. Instead, the placental tissue grows abnormally and produces very high levels of the pregnancy hormone hCG.
Partial molar pregnancy — A normal egg is fertilised by two sperm (or one sperm that duplicates itself). This creates a triploid embryo — one with 69 chromosomes instead of the normal 46. The embryo is always severely abnormal and cannot survive. Some placental tissue develops normally, alongside the molar changes.
How Common Is It?
Molar pregnancies are rare. In the UK and across Europe, the incidence is roughly 1 to 3 per 1,000 pregnancies (Sebire et al., 2005). Rates are higher in Southeast Asia — up to 9.9 per 1,000 pregnancies in some studies from Japan and South Korea — likely due to genetic and dietary factors (Bracken et al., 2023).
Between 2000 and 2009, England and Wales registered 5,793 patients with complete moles and 7,790 with partial moles (Savage et al., 2013). That's across a decade — but it's still a significant number of women navigating this diagnosis.
Risk factors include:
- Maternal age over 35 — risk increases 5-fold after age 40 (Matsui et al., 2003)
- Previous molar pregnancy — recurrence risk is roughly 1-2% after one molar pregnancy (Eagles et al., 2015)
- History of miscarriage — particularly recurrent miscarriage
- Diet low in carotene — some studies link low vitamin A intake to higher risk, though evidence is mixed
Signs and Symptoms
One of the cruel things about molar pregnancy is that the early signs can look exactly like a normal — even a healthy — pregnancy. You might get a positive test, feel nauseous, even have a growing belly. The difference is that things aren't progressing as they should.
I know this part can be really worrying to read — I've been there myself. Common symptoms of complete molar pregnancy:
- Vaginal bleeding, often dark brown or bright red, in the first trimester
- Severe nausea and vomiting (hyperemesis gravidarum) — your hCG levels are extremely high
- Uterus growing faster than expected for your dates
- No fetal heartbeat on scan
- Passing grape-like tissue
- High blood pressure very early in pregnancy
I know this part can be really worrying to read — I've been there myself. Common symptoms of partial molar pregnancy:
- Symptoms often resemble a miscarriage — bleeding, cramping
- The uterus may be smaller than expected
- A fetal heartbeat may be detected, but it will stop
- Symptoms are often milder and harder to distinguish from a normal miscarriage
If you're experiencing any of these, please contact your GP or early pregnancy unit. They're trained to investigate this properly.
How Is It Diagnosed?
A molar pregnancy is usually picked up during an early ultrasound scan. The sonographer may see:
On ultrasound:
- Complete mole: a "snowstorm" or "cluster of grapes" pattern — cystic structures filling the uterus with no embryo visible
- Partial mole: an abnormal embryo with placental cysts, or what looks like a missed miscarriage with unusual placental appearance
Blood tests (hCG): hCG levels are typically very high with complete moles — sometimes well above the normal range for the gestational age. With partial moles, hCG may be only moderately elevated.
Final diagnosis comes after the tissue is removed and examined under a microscope (histopathology). This is the definitive test and takes a few days to come back.
Treatment: What Happens Next
From what I've learned working with families going through this, the treatment process is very well-established. The primary treatment for a molar pregnancy is removal of all abnormal tissue. This is typically done through a surgical procedure called dilation and curettage (D&C).
The D&C Procedure
You'll be given either general or local anaesthetic, and the doctor will gently dilate your cervix and remove the molar tissue using suction. The procedure usually takes 15 to 30 minutes and is performed as a day case — meaning you can go home the same day.
The removed tissue is sent to a lab for histopathological examination, which confirms the diagnosis and determines whether it was complete or partial.
When Hysterectomy May Be Considered
If you've completed your family and don't want further pregnancies, your doctor may discuss hysterectomy (removal of the uterus) as an option. This eliminates the risk of persistent disease but is a major surgery — it's not a first-line treatment for most women.
The Follow-Up Period: hCG Monitoring
This is the part that often feels the longest and most stressful. After a D&C, your blood hCG levels need to be monitored regularly to make sure all the molar tissue has been removed and nothing is growing back.
The monitoring process:
- Blood or urine tests every 1-2 weeks until hCG falls to zero
- After hCG normalises: monthly tests for 6 months (complete mole) or 3 months (partial mole)
- Effective contraception is essential during this period — pregnancy would make hCG monitoring impossible
For most women, hCG drops to zero within 8 to 12 weeks. But for some, it takes longer — and that's completely normal. The pace depends on how high your hCG was at the start.
Why contraception matters: Your doctor will recommend reliable contraception (the combined pill or progestogen-only methods are usually fine) because you cannot get pregnant during the monitoring period. A new pregnancy would produce hCG and make it impossible to know if your levels are falling for the right reasons.
What If hCG Doesn't Fall?
In about 15-20% of complete molar pregnancies and 1-5% of partial molar pregnancies, hCG levels don't fall to zero — or they start rising again. This suggests the molar tissue is still growing, and it's called gestational trophoblastic neoplasia (GTN).
I know "neoplasia" sounds scary. But here's what matters: GTN is one of the most treatable forms of abnormal cell growth in medicine. It responds extremely well to chemotherapy.
Treatment for GTN:
- Low-risk GTN: usually treated with single-agent chemotherapy (methotrexate or actinomycin D) — cure rate is nearly 100%
- High-risk GTN: requires combination chemotherapy — cure rate is still over 90%
From what I've learned working with families going through this, the treatment process is very well-established. The Christie NHS Foundation Trust in Manchester is the UK's specialist centre for gestational trophoblastic disease. They track hCG results for every patient in England and Wales and coordinate treatment. Your follow-up results are automatically sent to them (Seckl et al., 2013).
Emotional Recovery
This is the part that doesn't get enough airtime. You were pregnant. You might have had a name, a due date, maybe told people. And now you're being told it wasn't a real pregnancy — that it was something else entirely. That's a unique kind of grief.

You might feel:
- Confused — "Was I ever really pregnant?"
- Guilt — "Did I cause this?" (You didn't.)
- Anger — at the unfairness of it all
- Fear — about what this means for future pregnancies
- Loneliness — because most people haven't heard of molar pregnancy and don't understand
All of these feelings are valid. You don't have to "get over it" on anyone else's timeline. Take the space you need.
The Miscarriage Association (UK) has a dedicated molar pregnancy support service, and they've been incredibly helpful for the women I've worked with. The GTD (Gestational Trophoblastic Disease) support network run by The Christie is another excellent resource.
Pregnancy After a Molar Pregnancy
This is the question everyone asks: Can I get pregnant again?
Yes. Absolutely. And here's the reassuring data:
Most women have normal pregnancies after a molar pregnancy. The recurrence risk is approximately 1-2% after one molar pregnancy, rising to about 15-20% after two (Berkowitz & Goldstein, 2009). So after one molar pregnancy, your chances of a normal pregnancy next time are excellent.
Research from the Trophoblastic Disease Registry found that viable pregnancy outcomes were achieved in 65% of women who conceived after a complete molar pregnancy and 83% after a partial molar pregnancy (Garrett et al., 2008).
Your doctor will likely recommend:
- Waiting until hCG monitoring is complete and you've had the all-clear
- An early ultrasound in your next pregnancy (usually at 6-7 weeks) to confirm everything is developing normally
- Monitoring hCG again after delivery to be absolutely certain
That extra monitoring in your next pregnancy can actually be reassuring — you'll get to see your baby earlier and more often than most.
The Bottom Line
A molar pregnancy is a frightening diagnosis, but it's one that modern medicine handles well. The tissue is removed, your hCG is monitored, and in the rare cases where something persists, chemotherapy is highly effective. The vast majority of women who've had a molar pregnancy go on to have healthy babies.
Give yourself permission to grieve what was lost. This wasn't just a medical event — it was the loss of a pregnancy you were hoping for. Let yourself feel whatever comes up, and lean on the support that's available. You don't have to navigate this alone.
Frequently Asked Questions
▸Is a molar pregnancy the same as a miscarriage?
No. A miscarriage is the loss of a normally developing pregnancy. A molar pregnancy is an abnormal growth from the start — no viable embryo forms. The tissue is abnormal at a genetic level. The emotional impact may be similar, but medically they're very different conditions with different treatment and monitoring needs.
▸Can a molar pregnancy be missed on ultrasound?
Complete molar pregnancies are usually quite distinctive on ultrasound — the "cluster of grapes" pattern is hard to miss. Partial moles, however, can look very similar to a missed miscarriage, and the molar component may not be obvious until histopathology after the tissue is removed. This is why post-D&C lab analysis is so important.
▸How long do I have to wait before trying to conceive again?
After a complete molar pregnancy, you'll need hCG monitoring for approximately 6 months. After a partial mole, it's usually 3 months. Once your hCG has been confirmed at zero for the required period, most doctors recommend waiting a further 6 months before trying to conceive — so roughly 12 months total for complete moles. Your specialist will advise based on your individual situation.
▸Does a molar pregnancy mean I'm more likely to get cancer?
A molar pregnancy itself isn't cancer, but it can develop into gestational trophoblastic neoplasia (GTN), which is a type of abnormal cell growth. About 15-20% of complete moles and 1-5% of partial moles progress to GTN. The good news: GTN is one of the most curable forms of abnormal cell growth, with cure rates above 95% with chemotherapy. The hCG monitoring is specifically designed to catch this early.
▸Is it safe to get pregnant while on contraception during monitoring?
No. Effective contraception is essential during the monitoring period. If you became pregnant, your body would produce hCG, making it impossible to tell whether your hCG levels are falling properly or rising due to persistent molar tissue. Most doctors recommend the combined pill or progestogen-only pill during this time. Barrier methods alone aren't recommended because of the higher failure rate.
▸Can molar pregnancy happen with IVF?
Yes, though it's uncommon. Molar pregnancies can occur with IVF, including with donor eggs. The genetic error that causes a molar pregnancy can happen at fertilisation regardless of whether conception is natural or assisted. If you've had a molar pregnancy during IVF, your fertility clinic will work closely with the trophoblastic disease centre during monitoring.
References
- Sebire NJ, Foskett M, Fisher RA, et al. Risk of partial and complete hydatidiform molar pregnancy in relation to maternal age. BJOG. 2002;109(1):99-102. PubMed
- Savage P, Williams J, Short D, et al. The relationship of maternal age to molar pregnancy incidence, risks for chemotherapy and subsequent pregnancy outcome. J Reprod Med. 2013;58(1-2):53-58. PubMed
- Bracken MB, Eagle C, Kruger K. Molar pregnancy in the last 50 years: A bibliometric analysis of global research output. Placenta. 2021;107:14-21. ScienceDirect
- Matsui H, Iitsuka Y, Suzuka K, et al. Relationship of maternal age to molar pregnancy incidence and subsequent pregnancy outcomes. Gynecol Obstet Invest. 2003;56(2):110-113. PubMed
- Eagles N, Sebire NJ, Short D, et al. Risk of recurrent molar pregnancy and subsequent pregnancy outcome following complete or partial hydatidiform molar pregnancy. BJOG. 2015;122(4):527-533. PubMed
- Seckl MJ, Sebire NJ, Berkowitz RS. Gestational trophoblastic disease. Lancet. 2010;376(9742):717-729. PubMed
- Berkowitz RS, Goldstein DP. Current management of gestational trophoblastic diseases. Gynecol Oncol. 2009;112(3):654-662. PubMed
- Garrett LA, Garner EI, Feltmate CM, et al. Subsequent pregnancy outcomes after complete and partial molar pregnancy, recurrent molar pregnancy, and gestational trophoblastic neoplasia. J Reprod Med. 2008;53(11):828-834. PubMed
- NHS. Molar Pregnancy. NHS
- Cancer Research UK. Follow up after molar pregnancy. Cancer Research UK

Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional for diagnosis and treatment of any medical condition. If you are experiencing symptoms of a molar pregnancy, please contact your GP or nearest early pregnancy unit immediately.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











