How Your Thyroid Affects Fertility (And What to Eat About It)
Your thyroid controls ovulation, implantation, and early pregnancy. A nutritionist explains the numbers that matter, the foods that help, and the test your GP might be missing.


The gland nobody tells you about
When I started reading about fertility, everything pointed to ovaries — AMH, egg quality, follicle counts. Important, obviously. But it took me longer than it should have to understand that a small butterfly-shaped gland in my neck was just as involved in whether or not I'd get pregnant.
Your thyroid produces hormones (T3 and T4) that influence virtually every cell in your body, including your reproductive system. When it's working well, you don't notice it. When it's not, the effects can ripple through your cycle, your ovulation, your ability to implant, and your ability to hold a pregnancy — often without any obvious symptoms.
This is one of the most under-tested, under-discussed causes of fertility problems. And it's one of the most treatable.
How your thyroid affects fertility
Thyroid hormones are involved at almost every stage of conception and early pregnancy:
Ovulation. Hypothyroidism (underactive thyroid) can disrupt the regularity of your menstrual cycle by affecting the release of GnRH, which in turn suppresses the LH surge needed for ovulation. Some women with untreated hypothyroidism stop ovulating entirely. Others ovulate irregularly, making timing conception much harder.
The luteal phase. Even if you're ovulating, low thyroid function can shorten the luteal phase — the window between ovulation and your next period when a fertilised egg needs to implant. A luteal phase shorter than 10 days makes sustained implantation difficult.
Implantation. Thyroid hormones help regulate the endometrium (uterine lining). Insufficient thyroid function is associated with thinner endometrial lining and altered immune responses at the implantation site — both of which can prevent an embryo from establishing itself (Rao et al., 2020).
Early pregnancy maintenance. In the first 12 weeks, your baby depends entirely on your thyroid hormones — they can't produce their own yet. Subclinical hypothyroidism and thyroid autoimmunity (particularly Hashimoto's) are both associated with increased miscarriage risk. A 2024 ASRM guideline confirmed that thyroid antibodies (TPO antibodies) increase miscarriage risk even when TSH is technically within the normal range (ASRM, 2024).
Hyperprolactinaemia. Hypothyroidism can also raise prolactin levels. Elevated prolactin suppresses ovulation — it's the same mechanism that prevents ovulation during breastfeeding. Treating the thyroid often resolves this without needing separate medication.
The numbers that matter
Here's where it gets confusing. The "normal" TSH range for the general population is typically 0.4–4.0 mIU/L. But for fertility and pregnancy, that upper limit is too high.
| TSH Level (mIU/L) | General Status | Fertility Significance |
|---|---|---|
| Below 0.4 | Low — possible hyperthyroidism | May need investigation. Overactive thyroid also affects fertility. |
| 0.4–2.5 | Normal | Optimal range for conception and early pregnancy. |
| 2.5–4.0 | Normal (general population) | Suboptimal for fertility. Many specialists would treat at this level. |
| Above 4.0 | Elevated — subclinical hypothyroidism | Treatment strongly recommended before conception. |
| Above 10 | Overt hypothyroidism | Requires treatment. Associated with anovulation and pregnancy complications. |
Sources: ASRM 2024 Guidelines, RCOG Green-top Guideline No. 76, ATA Guidelines (Alexander et al., 2017).
The key takeaway: a TSH below 2.5 mIU/L is the target for women trying to conceive. The 2025 RCOG guideline and the 2024 ASRM guideline both recommend treating women with subclinical hypothyroidism (TSH above 4.0) with levothyroxine before conception, with a goal of reaching TSH ≤ 2.5 (Chan et al., 2025).
If you've been trying to conceive and your TSH is between 2.5 and 4.0, it's worth having a conversation with your GP or fertility specialist. You may not meet the general threshold for treatment, but many reproductive endocrinologists would consider it worth addressing.
Hashimoto's: when your immune system attacks your thyroid
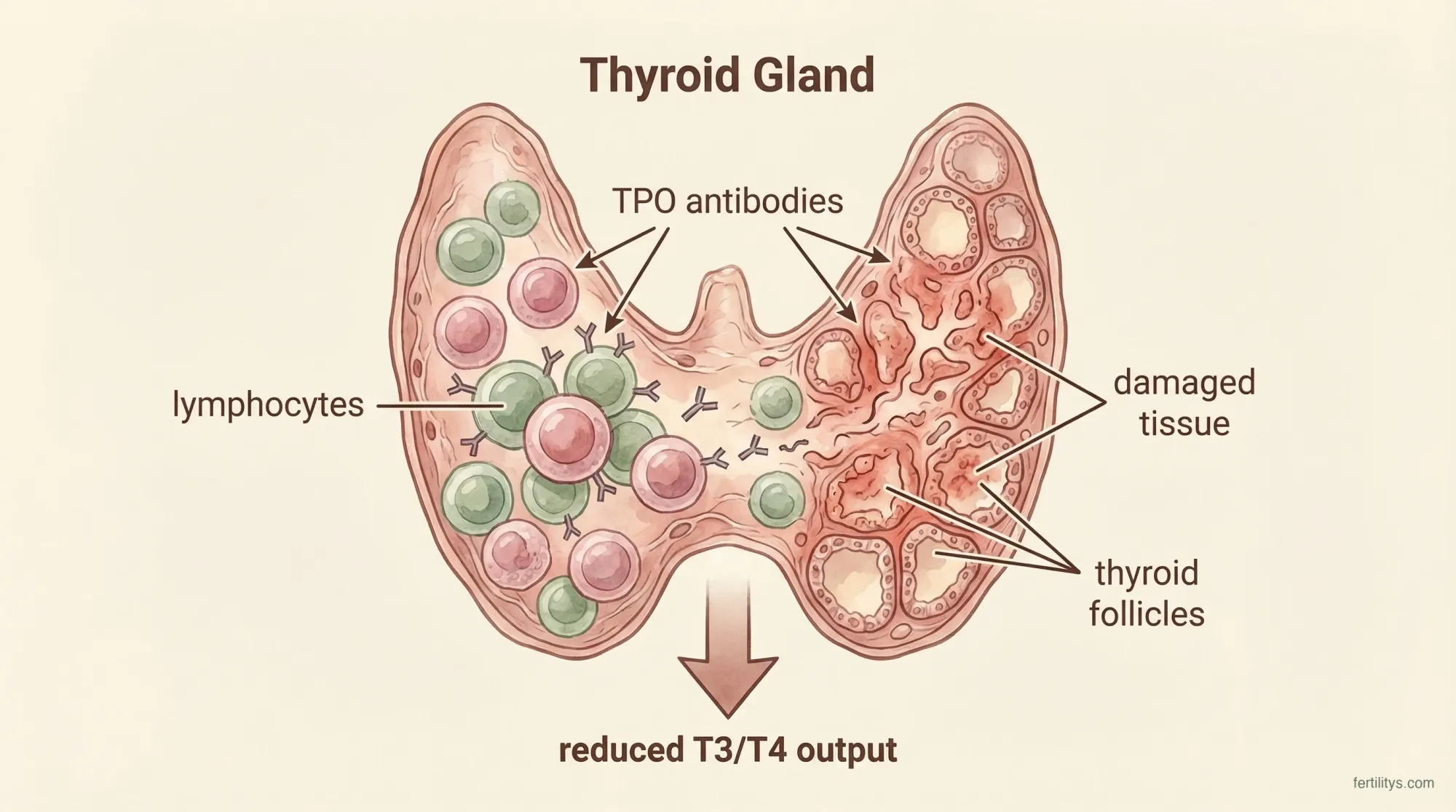
How Hashimoto's works: your immune system produces TPO antibodies that attack the thyroid gland, gradually reducing its ability to produce T3 and T4 hormones.
Hashimoto's thyroiditis is the most common cause of hypothyroidism in the UK. It's an autoimmune condition where your immune system produces antibodies (anti-TPO and anti-thyroglobulin) that gradually damage the thyroid gland.
What makes Hashimoto's particularly relevant for fertility is that the antibodies themselves may cause problems — independent of your TSH level. The 2024 ASRM guideline found evidence that women with thyroid autoimmunity (positive TPO antibodies) had increased miscarriage rates even when their TSH was normal (ASRM, 2024).
If you have Hashimoto's and are trying to conceive:
- Get your TSH checked regularly — Hashimoto's causes thyroid function to fluctuate, especially during periods of immune flare
- Aim for TSH ≤ 2.5 — even if your GP says your levels are "fine" based on the general range
- Request TPO antibody testing if it hasn't been done — knowing your antibody status helps your specialist plan your care
- Once pregnant, your levothyroxine dose typically needs to increase by 20–30% in the first trimester. Don't wait for a routine appointment — get tested as soon as you know you're pregnant
What to eat for your thyroid
This is where I can be most useful, because thyroid health is genuinely responsive to nutrition. The evidence supports focusing on these key nutrients:
Selenium — the most researched nutrient for thyroid autoimmunity. A 2024 meta-analysis of randomised controlled trials found that selenium supplementation significantly reduced TPO antibody levels in Hashimoto's patients (Santos et al., 2024). The recommended intake is 55–70 micrograms daily. Just 2–3 Brazil nuts provide about 200 micrograms — though levels vary widely, so don't rely on them as your only source.
- Best sources: Brazil nuts (1–3 daily), fish, shellfish, eggs, sunflower seeds, mushrooms
Iodine — essential for thyroid hormone production. Your thyroid literally can't make T3 and T4 without it. The UK doesn't fortify salt with iodine (unlike many countries), so mild deficiency is common, particularly in women who don't eat dairy or fish.
- Best sources: dairy (milk, yoghurt, cheese), fish, seaweed (but be cautious — some seaweed contains extremely high levels that can worsen thyroid problems), eggs
- NHS recommendation in pregnancy: 150 micrograms daily. Most prenatal vitamins don't contain enough — check the label
Iron — iron deficiency impairs thyroid hormone synthesis. If you're low in iron, your thyroid can't function optimally even if your iodine and selenium are fine. This is particularly relevant because iron deficiency is so common in women of reproductive age.
Zinc — involved in the conversion of T4 (the inactive form) to T3 (the active form). Good sources include red meat, shellfish, chickpeas, and pumpkin seeds.
Vitamin D — deficiency is common in both Hashimoto's and in people living in the UK generally. We've written a full article on vitamin D and fertility — it's worth reading alongside this one.
Foods to be cautious with
There's a lot of misinformation online about "thyroid-damaging foods." Here's what the evidence actually says:
- Cruciferous vegetables (broccoli, cauliflower, kale, cabbage) — these contain goitrogens that can theoretically interfere with iodine uptake, but only in very large quantities or when iodine intake is already low. Normal portions, especially cooked, are absolutely fine and shouldn't be avoided. The nutritional benefits far outweigh any theoretical risk
- Soy — may interfere with levothyroxine absorption if consumed at the same time. If you take thyroid medication, separate it from soy foods by at least 4 hours. Soy itself doesn't cause thyroid problems in people with adequate iodine
- Gluten — there's an association between coeliac disease and Hashimoto's (shared autoimmune mechanisms). If you have Hashimoto's and persistent gut symptoms, ask your GP about coeliac screening. But there's no evidence that going gluten-free helps thyroid function in people who don't have coeliac disease

Getting tested: what to ask for
A basic thyroid screen is a simple blood test. But "basic" often means just TSH — and that's not always enough. If you're trying to conceive or have been struggling, ask for:
- TSH — the first-line test. Most important single number.
- Free T4 (fT4) — how much active thyroid hormone is available. Can be low even when TSH is "normal"
- Free T3 (fT3) — less commonly tested but useful if you have symptoms despite normal TSH and fT4
- TPO antibodies — checks for Hashimoto's/thyroid autoimmunity. This is the test most commonly missed, and it's one of the most important for fertility
- Thyroglobulin antibodies — sometimes tested alongside TPO for a fuller picture
If your GP only tests TSH and says it's normal, but your TSH is above 2.5 and you've been struggling to conceive — push for the full panel. You're entitled to advocate for yourself, and a fertility specialist will want to see these numbers anyway.
🌿 Dani Recommends
A thyroid-friendly breakfast bowl
Two scrambled eggs (iodine + selenium + vitamin D), a handful of sautéed spinach (iron + zinc), half an avocado (healthy fats for hormone absorption), and 2 chopped Brazil nuts on top (selenium). Takes 10 minutes, covers four of the key thyroid nutrients in one meal, and tastes genuinely good. I eat some version of this most mornings — it's the kind of small, consistent choice that adds up over months.
The bottom line
Your thyroid is a small gland with an outsized impact on your fertility. Subclinical hypothyroidism and thyroid autoimmunity are common, often undiagnosed, and directly linked to difficulty conceiving, miscarriage, and pregnancy complications. The good news is that treatment — whether medication, nutrition, or both — is effective, affordable, and well-understood.
If you haven't had your thyroid checked, get it done. If you've been told your levels are "normal" but you're above 2.5 and struggling, question it. And if you have Hashimoto's, know that it absolutely doesn't mean you can't have a healthy pregnancy — it just means your thyroid needs a bit more attention than most.
What TSH level is best for getting pregnant?
Most fertility specialists recommend a TSH below 2.5 mIU/L for women trying to conceive. This is lower than the general population "normal" range of 0.4–4.0. The 2024 ASRM guideline and 2025 RCOG guideline both support treatment with levothyroxine for women with subclinical hypothyroidism (TSH above 4.0) who are trying to conceive.
Can hypothyroidism cause infertility?
Yes. Hypothyroidism can prevent ovulation, shorten the luteal phase, thin the endometrial lining, raise prolactin levels, and increase miscarriage risk. Even mild (subclinical) hypothyroidism can affect fertility. The good news is that treatment with levothyroxine is effective and well-tolerated.
Does Hashimoto's affect fertility?
Hashimoto's thyroiditis can affect fertility in two ways: through hypothyroidism itself, and through the thyroid antibodies (anti-TPO), which may independently increase miscarriage risk even when TSH is normal. Women with Hashimoto's should aim for a TSH below 2.5 and have their levels monitored closely during pregnancy.
What foods support thyroid health for fertility?
Focus on selenium (Brazil nuts, fish, eggs), iodine (dairy, fish, seaweed in moderation), iron (red meat, spinach, lentils), zinc (shellfish, pumpkin seeds), and vitamin D (oily fish, supplements). Normal amounts of cruciferous vegetables are fine — don't avoid broccoli or kale based on internet myths.
Should I get my thyroid tested before trying to conceive?
Yes — especially if you have a family history of thyroid problems, autoimmune conditions, irregular periods, or previous miscarriages. Ask for TSH, free T4, and TPO antibodies at minimum. A full thyroid panel gives your GP or fertility specialist the information they need to optimise your levels before you start trying.
References
- ASRM. (2024). Subclinical hypothyroidism in the infertile female population: a guideline. Fertility and Sterility, 121(4). ASRM
- Chan, S.Y. et al. (2025). Management of Thyroid Disorders in Pregnancy (RCOG Green-top Guideline No. 76). BJOG. Wiley
- Rao, M. et al. (2020). Role of hypothyroidism and associated pathways in pregnancy and infertility. Frontiers in Endocrinology. PMC
- Santos, L.R. et al. (2024). Selenium Supplementation in Patients with Hashimoto Thyroiditis: A Systematic Review and Meta-Analysis of RCTs. Thyroid. PMC
- Alexander, E.K. et al. (2017). 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy. Thyroid, 27(3), 315–389. PubMed
- NICE. (2019). Thyroid disease: assessment and management (NG145). NICE
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. Thyroid conditions require proper medical diagnosis and monitoring. Do not adjust thyroid medication without consulting your doctor. If you suspect a thyroid problem, see your GP for blood tests. Always consult a healthcare professional for advice specific to your situation.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











