Luteal Phase Symptoms: What's Normal, What's Not, and When to See a Doctor
What your body does after ovulation — and what those symptoms really mean.


💡 Quick Answer
The luteal phase is the second half of your menstrual cycle, lasting roughly 11–17 days between ovulation and your period. Common symptoms include breast tenderness, bloating, mood changes, fatigue, and mild cramping — all driven by rising progesterone levels. A luteal phase shorter than 10 days may affect fertility and is worth discussing with your doctor.
Key Takeaways
- The luteal phase begins immediately after ovulation and ends when your period starts — typically lasting 12–14 days
- Progesterone is the dominant hormone during this phase, and it's responsible for most of the symptoms you feel
- Luteal phase symptoms overlap significantly with early pregnancy signs, which is why the two-week wait can feel so confusing
- A short luteal phase (under 10 days) may indicate luteal phase deficiency, which can affect your ability to conceive
- Nutrition, stress management, and certain supplements may help support a healthy luteal phase
What Is the Luteal Phase?
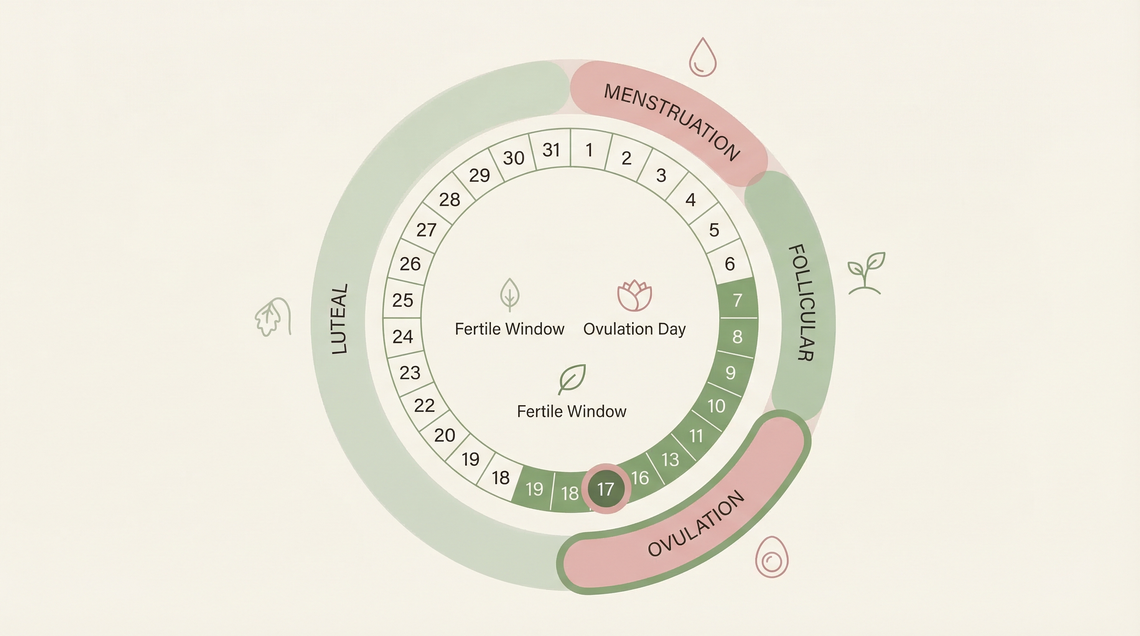
The luteal phase is the second half of your menstrual cycle — the stretch of days between ovulation and the start of your next period. It gets its name from the corpus luteum, a temporary structure that forms in your ovary from the follicle that released your egg.
Your menstrual cycle has two main halves. The follicular phase comes first, running from day one of your period through to ovulation. The luteal phase picks up from there. While the follicular phase can vary quite a bit in length from cycle to cycle, the luteal phase tends to be more consistent — usually between 12 and 14 days, though anything from 11 to 17 days is considered within normal range (Sonntag et al., 2023, Human Reproduction; ASRM Committee Opinion, 2021).
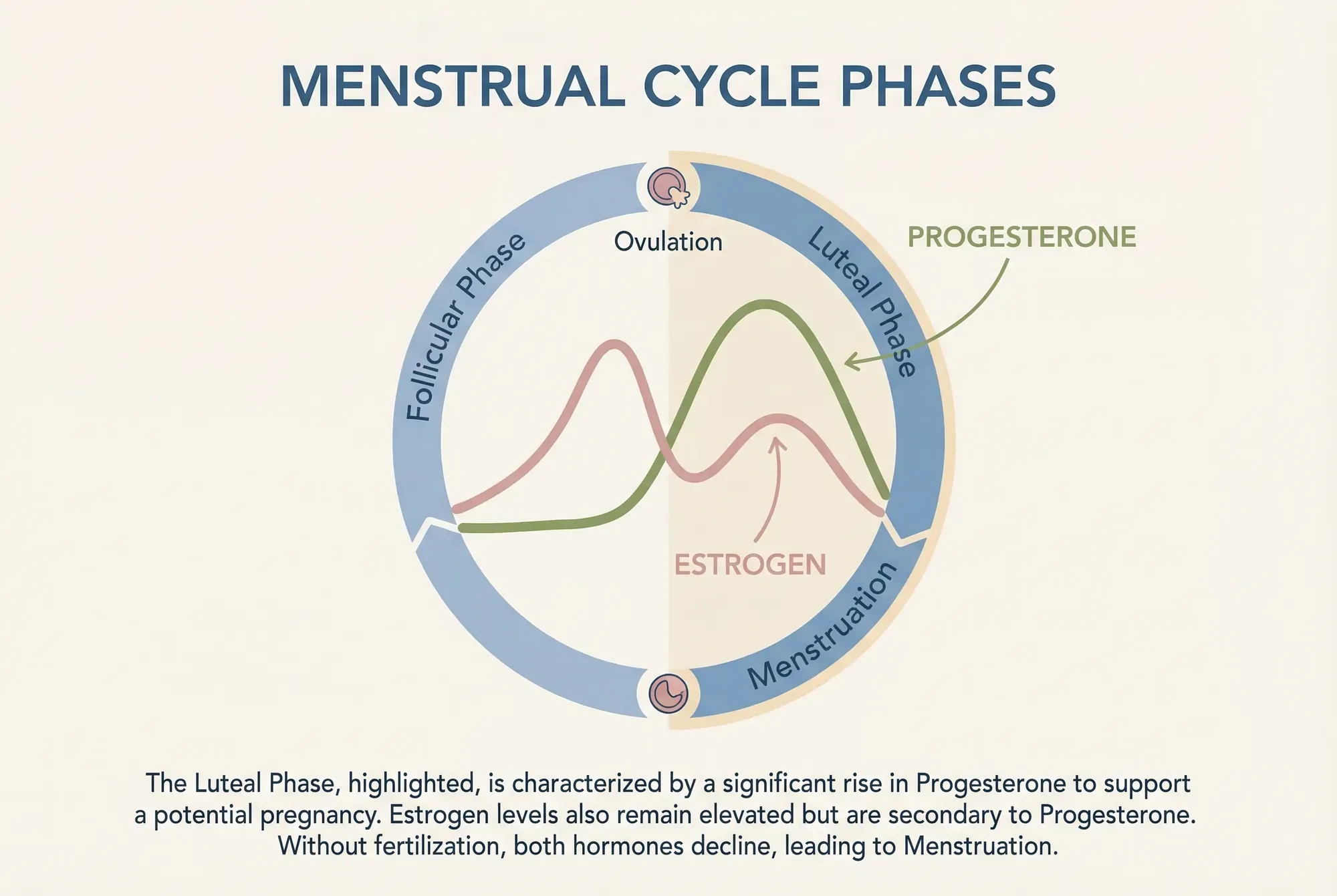
Here's what happens biologically: after ovulation, the empty follicle transforms into the corpus luteum and starts producing progesterone. This progesterone thickens the uterine lining (endometrium), preparing the uterus as a supportive environment for a fertilised egg to implant. If pregnancy doesn't occur, the corpus luteum breaks down after roughly 10–14 days, progesterone levels drop, and the uterine lining sheds — that's your period.
"I think of the luteal phase as your body's 'preparation window.' It's doing incredible work behind the scenes, regardless of whether pregnancy happens that cycle. Understanding what your body is going through can make those symptoms feel a lot less mysterious." — Danielle Bowen, MSc, RNutr
Common Luteal Phase Symptoms
Progesterone is the driving force behind most luteal phase symptoms. It peaks around 6–8 days after ovulation (approximately day 21 of a 28-day cycle) and can affect everything from your breasts to your bowels to your brain (Schmalenberger et al., 2021, Psychoneuroendocrinology).
Not everyone experiences all of these, and they can vary in intensity from cycle to cycle. But here are the most common ones:
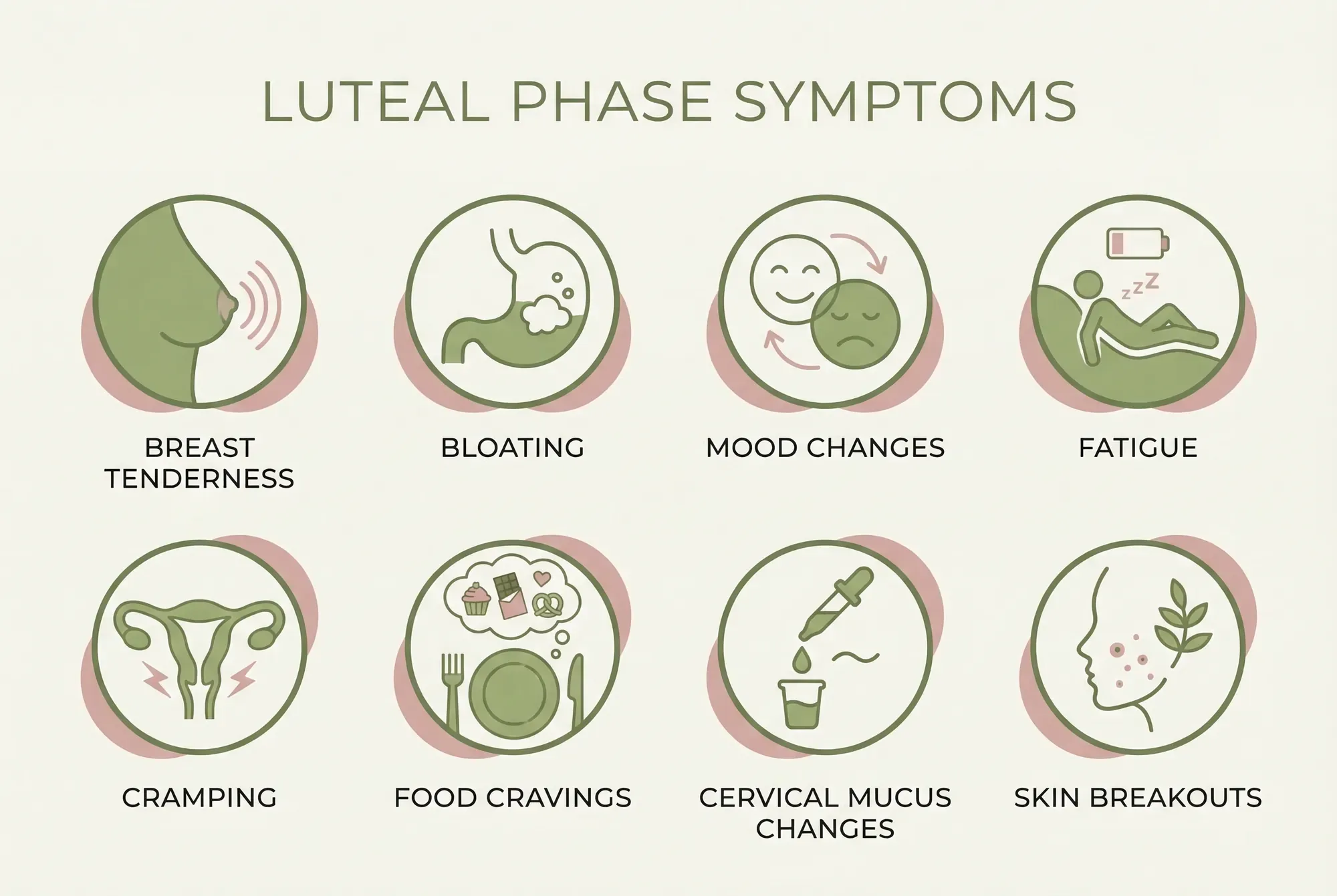
Breast Tenderness and Swelling
Breast tenderness is one of the earliest and most common luteal phase symptoms. Rising progesterone stimulates breast tissue growth and fluid retention, making your breasts feel heavier, swollen, or sore to touch. A 2025 prospective study published in PMC found that breast tenderness was significantly more common in ovulatory cycles with a normal luteal phase compared to anovulatory cycles — suggesting it's actually a sign your hormones are doing what they should (Prior et al., 2025).
This typically starts 3–5 days after ovulation and resolves once your period begins and progesterone drops.
Bloating and Water Retention
That uncomfortable puffiness around your abdomen? Progesterone slows down your digestive system and promotes water retention. Research by Dennerstein et al. (2011) found that bloating was among the most commonly reported physical symptoms across the luteal phase, affecting an estimated 65–75% of menstruating women to some degree.
You might notice your jeans feel tighter, your rings fit differently, or the number on the scale goes up by 1–2 kg. This is temporary water weight, not fat gain.
Mood Changes
The relationship between the luteal phase and mood is well-documented. Progesterone and its metabolite allopregnanolone interact with GABA receptors in the brain — the same system targeted by anti-anxiety medications. For most women, this produces a mild calming effect. But for others, particularly those sensitive to hormonal fluctuations, it can trigger mood swings — irritability, anxiety, tearfulness, or persistent low mood (Schmalenberger et al., 2021).
Around 5–8% of menstruating women experience these mood changes at a clinical level — a condition called premenstrual dysphoric disorder (PMDD), which is distinct from typical PMS (premenstrual syndrome) (Epperson et al., 2012, Neuropsychopharmacology). If your mood symptoms consistently interfere with your daily life during the luteal phase, it's worth speaking with your GP or a mental health professional.
Fatigue and Sleep Changes
Feeling unusually tired in the second half of your cycle isn't in your head. Progesterone has a mild sedative effect — it quite literally makes you sleepier. Research has found that sleep architecture changes during the luteal phase, with reduced REM sleep and increased wakefulness during the night (Baker & Driver, 2007).
Your basal body temperature also rises by approximately 0.2–0.5°C after ovulation due to progesterone's thermogenic effect. This slight temperature increase can contribute to feeling warmer and less comfortable at night.
Mild Cramping
Light cramping during the luteal phase is normal and can have several causes. Around 6–12 days after ovulation, some women notice what's called implantation cramping — though this is more commonly reported than scientifically confirmed. General pelvic awareness and mild uterine contractions driven by prostaglandins are more likely explanations for luteal phase cramping.
Cramping that becomes severe, persistent, or is accompanied by heavy bleeding is not typical and warrants medical attention.
Appetite Changes and Food Cravings
There's a biological reason you want chocolate in the second half of your cycle. Research published in European Journal of Nutrition found that caloric intake increases by approximately 100–300 calories per day during the luteal phase compared to the follicular phase (Barr et al., 2018). Your metabolic rate genuinely increases slightly — your body is burning more energy to maintain the thickened uterine lining.
Cravings for carbohydrate-rich and high-fat foods are linked to the drop in serotonin that accompanies progesterone fluctuations.
Changes in Cervical Mucus
After the clear, stretchy, egg-white cervical mucus of your fertile window, luteal phase mucus becomes thicker, stickier, and less abundant. Some women notice a creamy white or slightly yellow discharge. This is progesterone at work — it thickens cervical mucus to create a barrier that protects a potential pregnancy.
Skin Changes
Breakouts during the luteal phase are common, particularly along the jawline and chin. Progesterone stimulates sebum production, and this increased oil output — combined with the normal shedding of skin cells — can clog pores. Acne that follows a cyclical pattern, appearing predictably in the week before your period, is often hormonally driven.
Luteal Phase Symptoms vs. Early Pregnancy: How to Tell the Difference
This is the question everyone in the two-week wait is asking. And unfortunately, the honest answer is: you often can't tell the difference based on symptoms alone.
The reason is straightforward. Whether you're pregnant or not, progesterone dominates the luteal phase and produces the same symptoms. Breast tenderness, fatigue, bloating, mild cramping, mood changes — these happen regardless of whether implantation occurred.
| Symptom | Normal Luteal Phase | Early Pregnancy |
|---|---|---|
| Breast tenderness | Resolves when period starts | May persist and intensify |
| Fatigue | Mild, improves with period | May increase over first trimester |
| Cramping | Mild, resolves | Mild, may continue intermittently |
| Nausea | Uncommon | Begins around weeks 5–6 |
| Basal body temp | Drops before period | Stays elevated |
| Missed period | Period arrives on schedule | Period doesn't arrive |
The most reliable early indicator is a sustained elevated basal body temperature (BBT) beyond 16–18 days past ovulation, followed by a positive pregnancy test. Home pregnancy tests are most accurate from the first day of your missed period — testing earlier increases the risk of false negatives.
What Is a Normal Luteal Phase Length?
A normal luteal phase lasts between 11 and 17 days, with most falling in the 12–14 day range (ASRM Committee Opinion, 2021, Fertility and Sterility). Unlike the follicular phase, which can vary significantly between cycles and between women, the luteal phase tends to be relatively consistent for each individual — usually varying by no more than 1–2 days from cycle to cycle.
You can estimate your luteal phase length by tracking ovulation (using OPK strips, BBT charting, or a fertility monitor) and counting the days until your period starts.
Short Luteal Phase: When to Be Concerned
A luteal phase lasting fewer than 10 days is considered short and may indicate luteal phase deficiency (LPD) — a condition where the corpus luteum doesn't produce enough progesterone, or doesn't produce it for long enough, to adequately support the uterine lining (ASRM, 2021).
LPD is a somewhat controversial diagnosis in reproductive medicine. The ASRM acknowledged in their 2021 committee opinion that while the condition exists, there's no single reliable test for diagnosing it, and its clinical significance is debated. However, a consistently short luteal phase — particularly in women trying to conceive — is worth investigating.
Potential causes of a short luteal phase include:
- Thyroid dysfunction — both hypothyroidism and hyperthyroidism can disrupt progesterone production
- Hyperprolactinaemia — elevated prolactin levels interfere with the hormonal signals that maintain the corpus luteum
- Excessive exercise — particularly in women with low body fat
- Polycystic ovary syndrome (PCOS) — although PCOS more commonly affects the follicular phase
- Stress — chronic stress raises cortisol, which can suppress progesterone production
- Perimenopause — luteal phases often shorten as women approach menopause
If you suspect a short luteal phase, your doctor may check mid-luteal progesterone levels (typically drawn 7 days after confirmed ovulation). Levels below 5 ng/mL may suggest inadequate progesterone production.
Supporting a Healthy Luteal Phase
While you can't directly control your corpus luteum, there are evidence-based ways to support healthy progesterone production and ease luteal phase symptoms.
Nutrition
"During the luteal phase, your metabolism actually increases slightly — your body is burning more energy. This is not the time to restrict calories. I encourage my clients to lean into warming, nutrient-dense foods and listen to their body's cues rather than fighting the cravings." — Danielle Bowen, MSc, RNutr

Foods that may support progesterone production:
- Zinc-rich foods — pumpkin seeds, chickpeas, lentils, cashews. Zinc is essential for the pituitary gland's production of follicle-stimulating hormone, which supports healthy ovulation and subsequent progesterone production (Nasiadek et al., 2020, Nutrients)
- Vitamin B6 — poultry, fish, potatoes, bananas. Some evidence suggests B6 may support progesterone levels, though large-scale studies are limited (Wyatt et al., 1999, BMJ)
- Vitamin C — citrus fruits, kiwi, peppers. A small 2003 study in Fertility and Sterility found that 750mg of vitamin C daily increased progesterone levels in women with luteal phase deficiency (Henmi et al., 2003)
- Complex carbohydrates — sweet potatoes, oats, brown rice. These help stabilise blood sugar, which in turn supports stable hormone production
- Magnesium — dark chocolate, leafy greens, almonds. Magnesium may help with bloating, mood, and sleep quality during the luteal phase (Parazzini et al., 2017, Archives of Gynecology and Obstetrics)
Lifestyle
- Moderate exercise — gentle movement like walking, yoga, or swimming can help with bloating and mood. Avoid overtraining, which can suppress progesterone
- Stress management — cortisol and progesterone compete for the same precursor hormone (pregnenolone), so chronic stress may reduce progesterone availability
- Sleep hygiene — prioritise 7–9 hours. Keep your bedroom cool to offset the temperature rise from progesterone
Supplements (Discuss With Your Healthcare Provider)
- Vitex agnus-castus (chasteberry) — some evidence suggests it may support luteal phase length and progesterone levels, particularly in women with mild hyperprolactinaemia (Westphal et al., 2006, Journal of Women's Health)
- Vitamin B6 — typically studied at 50–100mg daily for PMS symptom relief
- Magnesium glycinate — 200–400mg daily, particularly helpful for sleep and mood during the luteal phase
When to See a Doctor
Most luteal phase symptoms are normal and don't require medical attention. But see your GP or a fertility specialist if:
- Your luteal phase is consistently shorter than 10 days
- You experience severe mood symptoms that interfere with daily life (possible PMDD)
- You have been trying to conceive for 12+ months without success (or 6+ months if you're over 35)
- You notice significant mid-cycle bleeding (not spotting)
- Your symptoms have suddenly changed or worsened
Frequently Asked Questions
How do you feel during the luteal phase?
Most women notice breast tenderness, mild bloating, fatigue, and mood changes during the luteal phase. These are caused by rising progesterone levels after ovulation. Symptoms typically begin 3–5 days after ovulation and intensify in the days before your period. Not everyone experiences symptoms, and their severity can vary from cycle to cycle.
What should you avoid during the luteal phase?
There's no strict "avoid" list, but reducing caffeine intake may help with breast tenderness and anxiety, limiting salt can reduce water retention and bloating, and avoiding excessive alcohol is advisable as it can disrupt progesterone metabolism. If you're trying to conceive, it's wise to avoid smoking, recreational drugs, and excessive heat exposure (hot tubs, saunas) during this phase.
Can luteal phase symptoms tell you if you're pregnant?
Not reliably. Luteal phase symptoms and early pregnancy symptoms are driven by the same hormone — progesterone — and overlap significantly. The only reliable early indicators of pregnancy are a sustained elevated basal body temperature beyond 16–18 days past ovulation and a positive pregnancy test.
How long does the luteal phase last?
The average luteal phase lasts 12–14 days, though anywhere from 11 to 17 days is considered normal (ASRM, 2021). Unlike the follicular phase, your luteal phase length tends to be relatively consistent from cycle to cycle. A luteal phase shorter than 10 days may indicate luteal phase deficiency.
Is it normal to have no symptoms during the luteal phase?
Yes. Some women go through the luteal phase with minimal or no noticeable symptoms. This doesn't indicate a problem — it simply means you may be less sensitive to hormonal fluctuations. If you're ovulating regularly and your cycles are consistent, the absence of symptoms is nothing to worry about.
References
- ASRM Practice Committee (2021). Diagnosis and treatment of luteal phase deficiency: a committee opinion. Fertility and Sterility, 115(6), 1416–1423.
- Baker, F.C. & Driver, H.S. (2007). Circadian rhythms, sleep, and the menstrual cycle. Sleep Medicine, 8(6), 613–622.
- Barr, S.I. et al. (2018). Changes in macronutrient, micronutrient, and food group intakes throughout the menstrual cycle. European Journal of Nutrition, 57(Suppl 1), 65–72.
- Dennerstein, L. et al. (2011). Premenstrual symptoms: prevalence and relationship to baseline and prospective ratings. Journal of Women's Health, 20(5), 713–719.
- Epperson, C.N. et al. (2012). Premenstrual dysphoric disorder: evidence for a new category for DSM-5. American Journal of Psychiatry, 169(5), 465–475.
- Henmi, H. et al. (2003). Effects of ascorbic acid supplementation on serum progesterone levels in patients with a luteal phase defect. Fertility and Sterility, 80(2), 459–461.
- Nasiadek, M. et al. (2020). The role of zinc in selected female reproductive system disorders. Nutrients, 12(8), 2464.
- Parazzini, F. et al. (2017). Magnesium in the gynecological practice. Archives of Gynecology and Obstetrics, 296, 297–305.
- Prior, J.C. et al. (2025). Breast tenderness and swelling experiences related to menstrual cycles and ovulation. PMC.
- Schmalenberger, K.M. et al. (2021). A specific profile of luteal phase progesterone and premenstrual symptoms. Psychoneuroendocrinology, 125, 105107.
- Westphal, L.M. et al. (2006). Double-blind, placebo-controlled study of Fertilityblend. Journal of Women's Health, 15(3), 297–303.
The content on fertilitys.com is for informational and educational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your doctor or other qualified health provider with any questions you may have regarding a medical condition.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.