Low AMH: What It Means and What You Can Actually Do
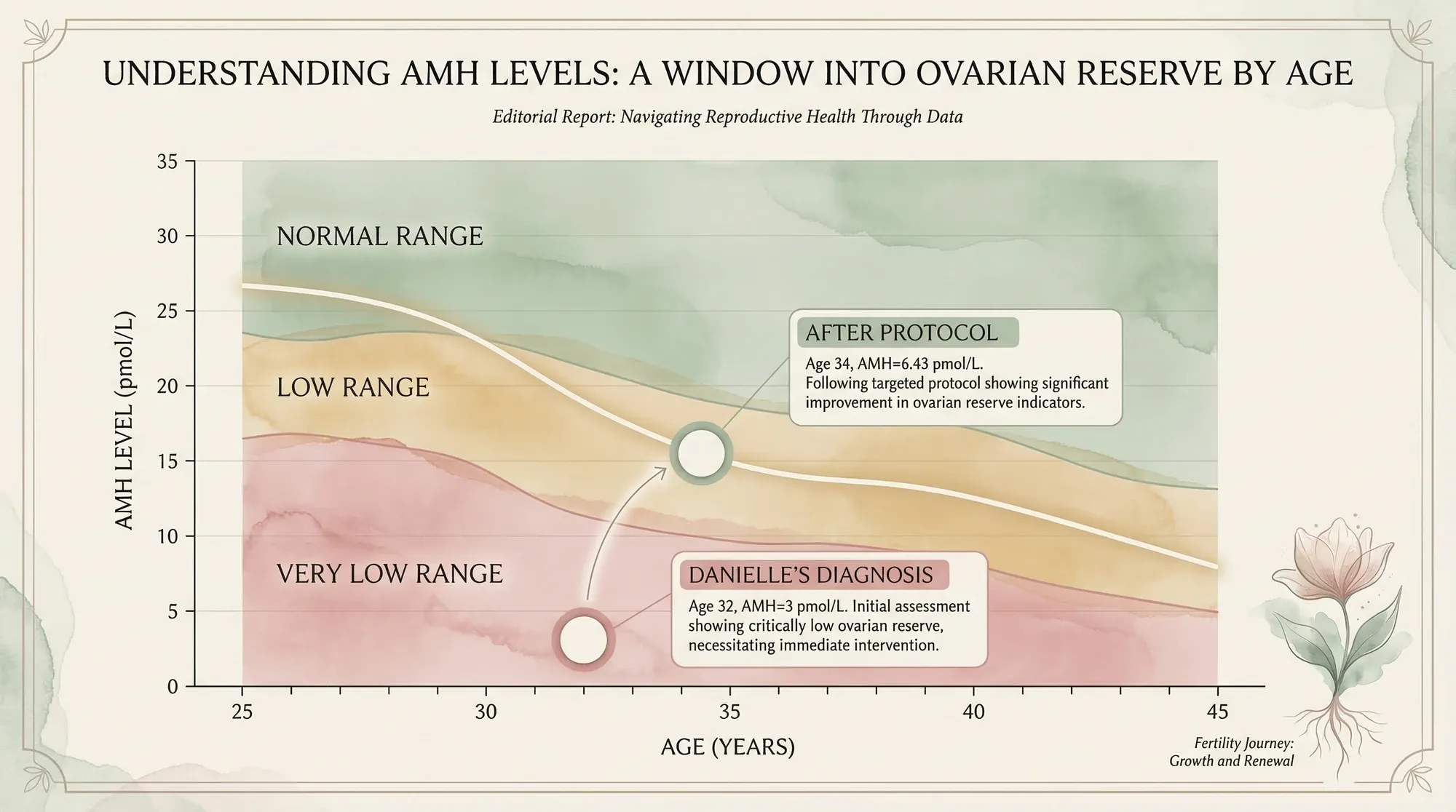
A registered nutritionist diagnosed with an AMH of 3 pmol/L shares the protocol that raised her levels to 6.43 and led to a natural pregnancy


When my AMH results came back at 3 pmol/L, I didn't understand what the number meant. I just knew from the look on the nurse's face that it wasn't good.
I was 32. A healthy AMH for my age should have been somewhere above 20 pmol/L. Mine was barely measurable. In clinical terms, my ovarian reserve — the estimated number of eggs I had left — looked like that of a woman a decade older.
The fear was instant and visceral. This sudden, overwhelming clarity that I wanted a family, paired with the feeling that it was already slipping away.
If you've just received a low AMH result, I want you to know something before we go any further: a low AMH number is not a sentence. It doesn't tell you whether you can get pregnant. It doesn't predict your future. And there is far more you can do about it than most clinics will ever tell you.
I know this because I lived it. My AMH rose from 3 to 6.43 pmol/L. I conceived naturally. And my son Bowie is proof that the numbers don't get the final word.
This is everything I wish someone had told me the day I got that result.
What Does Low AMH Actually Mean?
AMH — anti-Müllerian hormone — is a protein produced by the small developing follicles in your ovaries. The more follicles you have at any given time, the higher your AMH reading. So when a blood test shows low AMH, it's telling you that you have fewer developing follicles than average for your age.
But here's what the number doesn't tell you — and this is crucial:
- It doesn't measure egg quality — only how many follicles are developing
- It doesn't predict natural conception — a 2017 JAMA study of 750 women found no difference in pregnancy rates between low and normal AMH groups (Steiner et al., JAMA)
- It doesn't show the rate of decline — your level could have been low for years or dropped recently
- It can fluctuate between tests — seasonal variation, illness, and lab method all affect results
Think of AMH like a fuel gauge that shows how much petrol is in the tank, but tells you nothing about the condition of the engine. You could have a low reading and still be perfectly capable of getting where you need to go.
I remember sitting in the car park after getting my results, Googling 'AMH 3 pmol/L' on my phone. Every result that came up felt like a countdown clock. Forums full of women in the same panic. Clinic websites pushing egg freezing. Nobody — not one single source I found that day — told me what I'm telling you now: that this number is one piece of a much bigger puzzle. I wish someone had.
When I was diagnosed, nobody explained any of this to me. I was just handed a number and a referral for egg freezing. It took me months of researching the literature myself to understand that AMH is one piece of a much larger picture — and not even the most important piece.
What Counts as "Low"?
AMH is measured in pmol/L (common in the UK and Europe) or ng/mL (common in the US). To convert: 1 ng/mL = 7.14 pmol/L.
| Category | pmol/L | ng/mL | What It Suggests |
|---|---|---|---|
| High | > 35 | > 5.0 | Large follicle pool (may suggest PCOS) |
| Normal | 7–35 | 1.0–5.0 | Expected range for reproductive age |
| Low | 3.5–7 | 0.5–1.0 | Reduced ovarian reserve |
| Very low | < 3.5 | < 0.5 | Significantly diminished reserve |
My result of 3 pmol/L — about 0.42 ng/mL — put me firmly in "very low." At 32, it felt like a death sentence for my fertility dreams. But as I'd go on to learn, these categories are guidelines, not verdicts.
I spent the next week in a fog. I couldn't focus on my master's coursework. I cried in the shower where Tim couldn't hear me. I kept doing the maths in my head — if I started egg freezing immediately, at three rounds minimum, that was £15,000 to £21,000 with no guarantee it would work. And the whole time, a voice in my head kept saying: there has to be another way.
Low AMH and Fertility: What the Research Actually Shows
Here's what changed everything for me — and what I now share with every client who walks in with a low AMH result and terror in their eyes.
Low AMH does not reliably predict whether you'll conceive naturally.
I know that sounds too good to be true when you're staring at a number that puts you in the "very low" category. But the research is clear:
- A landmark 2017 JAMA study followed 750 women aged 30–44 who were actively trying to conceive. After 12 cycles, pregnancy rates were almost identical between women with low AMH and women with normal AMH (Steiner et al., 2017). The authors concluded that AMH should not be used to assess natural fertility.
- A 2021 meta-analysis of 4,388 women confirmed that AMH is a poor predictor of natural conception (Li et al., Frontiers in Endocrinology).
- A 2019 Cochrane Review found that while AMH predicts IVF response (how many eggs you'll retrieve), it does not predict whether IVF will result in a live birth (Iliodromiti et al., 2019).
What AMH does predict is how your ovaries will respond to stimulation drugs during IVF — which is why fertility clinics focus on it so heavily. They're looking through a treatment lens. But if you're trying to conceive naturally, or wondering whether you should even try, AMH alone shouldn't determine your decision.
💬 What I tell every client
When I sit with a woman who's just been told her AMH is low, the first thing I say is: "This number tells us about quantity, not quality. And quality is where we can make the biggest difference." I've had clients with AMH levels lower than mine who went on to conceive. I've also had clients with perfect AMH who struggled. The number is one data point — it's not your destiny.
One of my clients came to me last year with an AMH of 1.8 pmol/L at 35. She'd been told by two clinics that IVF was her only option. She was devastated — she and her partner had only just started trying. We worked together on a nutrition and lifestyle protocol for six months. She conceived naturally. Her baby is due this summer. I'm not telling you this to make promises — every woman's situation is different. But I am telling you that the research and my clinical experience consistently show that low AMH alone is not the fertility death sentence it's made out to be.
My Diagnosis: The Day Everything Changed
My fertility journey didn't start with trying to conceive. It started in December 2020, with a routine smear test.
The results showed pre-cancerous cells on my cervix — and this wasn't the first time. I'd already had the LLETZ procedure twice before, where the affected tissue is removed. This third treatment left my consultant concerned. My cervix was weakened and scarred, and another round could compromise my ability to carry a pregnancy. The advice was clear: if you want a family, don't wait too long.
But life doesn't align with biology on demand. Tim and I had only met in March 2020, just before lockdown. Our entire relationship had been shaped by restrictions. We hadn't done any of the things couples normally do before starting a family. We made the honest decision: it wasn't the right time yet.
Still, that consultant's warning stayed with me. So I booked a routine fertility blood test, expecting reassurance.
What I got was an AMH of approximately 3 pmol/L.
The clinics I consulted were direct. One told me egg freezing was my only realistic option. But with AMH this low, they said stimulation was unlikely to yield enough eggs in a single cycle — I'd probably need at least three rounds, at £5,000–£7,000 each. The financial burden was enormous. But it was what one doctor said next that made me walk away entirely.
"He told me that nutrition couldn't make any difference," I recall. "That if I wanted to preserve my fertility, I had to freeze my eggs. And I knew — from everything I was already learning in my master's degree — that wasn't the full truth."
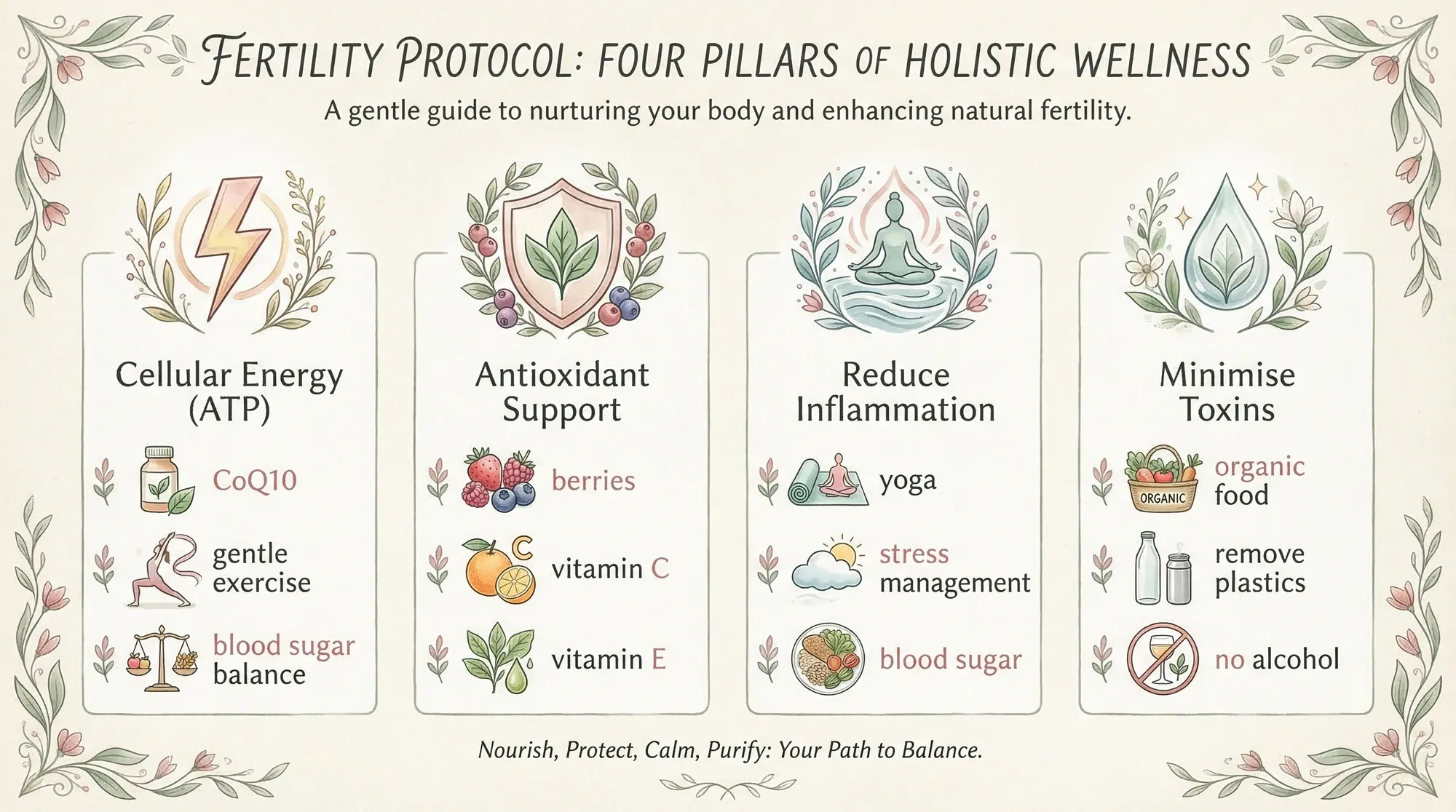
The 4-Pillar Protocol I Built Instead

By the time of my diagnosis, I was already studying for my master's in nutritional science. What I found in the research was a world away from the rigid messaging I'd received at the clinics. Study after study showed that nutrition and lifestyle interventions could improve egg quality, fertility treatment outcomes, and pregnancy rates. The evidence wasn't fringe — it was peer-reviewed and growing. But almost none of it was reaching women in consultation rooms.
So I did something that felt terrifying at the time. I stepped back from the clinics and built my own protocol.
I remember the exact moment it shifted from research to conviction. I was reading a paper on CoQ10 and mitochondrial function in oocytes during my master's degree, and something clicked. The clinics had told me there was nothing I could do about my egg reserve. But the research was telling me a completely different story — that while I couldn't create new eggs, I could fundamentally change the environment my existing eggs developed in. I could give them better energy, less oxidative damage, less inflammation, fewer toxins. I filled an entire notebook that week. By Friday, I had my protocol.
Pillar 1: Cellular Energy (ATP)
The energy available to your cells directly affects egg quality — eggs are among the most metabolically active cells in your body, and they need enormous amounts of ATP to divide properly. I made three key changes:
- CoQ10 at 200mg per day — a coenzyme that supports mitochondrial energy production. The landmark 2018 study by Ben-Meir et al. in Aging Cell showed CoQ10 supplementation improved oocyte quality in age-related decline.
- Switched from HIIT to gentle exercise — I'd been doing intense interval training, which I believe was driving excess cortisol and placing unnecessary stress on my body. I moved to yoga, walking, swimming, and fertility-specific acupuncture.
- Blood sugar stabilisation — I eliminated refined sugars and focused on balanced meals with protein, healthy fats, and complex carbohydrates at every sitting.
Giving up HIIT was genuinely hard. I'd been a CrossFit person for years — it was my stress release, my social life, my identity. Walking away felt like losing something. But I kept coming back to the cortisol research. High-intensity exercise floods your system with cortisol, and cortisol directly interferes with the hormones that recruit and develop follicles. I swapped it for yoga, long walks with our dog, and swimming. It took about three weeks before I stopped missing the intensity. And honestly? My body thanked me. My sleep improved. My cycles became more regular. I wish I'd made the switch years earlier.
Pillar 2: Antioxidant Support
Oxidative stress is one of the key drivers of egg quality decline. Every cell in your body produces free radicals as a byproduct of energy production, and your eggs are particularly vulnerable. I dramatically increased my intake of:
- Berries — blueberries, strawberries, raspberries (always organic for the Dirty Dozen)
- Vitamin C-rich foods — peppers, broccoli, kiwi, citrus
- Vitamin E-rich foods — almonds, sunflower seeds, avocado
- Dark leafy greens — spinach, kale, chard (organic)
The 2018 JAMA study of 325,639 women found that higher organic food consumption was associated with significantly lower cancer risk (Baudry et al., JAMA Internal Medicine) — and for fertility specifically, the Harvard EARTH study showed women eating high-pesticide produce had 18% fewer eggs retrieved during IVF and 26% lower odds of live birth (Chiu et al., 2018).
Pillar 3: Reduce Inflammation
Chronic low-grade inflammation quietly undermines reproductive health. It's invisible — you can't feel it — but it affects everything from implantation to early pregnancy. I addressed it through:
- Blood sugar regulation — insulin spikes trigger inflammatory cascades
- Stress management — weekly yoga, regular fertility acupuncture, eight hours of sleep every night (non-negotiable)
- Omega-3 fatty acids daily — from oily fish and a high-quality supplement
- Mediterranean dietary pattern — shown by Karayiannis et al. (2018) to improve IVF success rates by up to 40%
Pillar 4: Minimise Toxin Exposure
Endocrine disruptors — chemicals that mimic or interfere with your hormones — are everywhere. BPA in plastic containers, phthalates in fragrances, pesticides on food, parabens in skincare. Each individual exposure might be tiny, but the cumulative load matters enormously when you're trying to optimise egg quality.
- Removed all plastics from my kitchen — glass and stainless steel only
- Stopped drinking alcohol completely — even "moderate" drinking affects oocyte maturation (Fan et al., 2017)
- Switched to organic wherever possible — especially the Dirty Dozen
- Eliminated synthetic fragrances — perfume, scented candles, air fresheners
- Clean skincare and cleaning products — I checked every label
The toxin audit was eye-opening. Tim came home one evening to find me sitting on the bathroom floor surrounded by every product we owned — shampoo, deodorant, face cream, cleaning sprays, candles. I was going through each one on an app that scans ingredients for endocrine disruptors. More than half of them went in the bin. The scented candles I loved? Gone — synthetic fragrances are one of the most common sources of phthalates in the home. Our Tupperware? Replaced with glass. It felt extreme at the time. But when you understand that these chemicals literally mimic oestrogen in your body and can disrupt the precise hormonal signalling that your eggs need to develop properly, it stops feeling extreme and starts feeling obvious.

My Supplement Protocol
Supplements supported my food-first approach — they didn't replace it. But for low AMH specifically, the evidence on certain supplements is compelling enough that I consider them essential:
| Supplement | My Dose | Why | Key Evidence |
|---|---|---|---|
| CoQ10 (ubiquinol) | 200mg/day | Mitochondrial energy for egg cells | Ben-Meir et al. 2018, Aging Cell |
| Vitamin D | 10mcg/day | Hormone regulation, follicle development | Chu et al. 2018, Human Reproduction |
| Omega-3 (EPA/DHA) | Daily | Anti-inflammatory, blood flow to ovaries | Gaskins & Chavarro 2018, Fertility & Sterility |
| Wild Nutrition fertility multi | As directed | Methylfolate, zinc, B12, iodine | Food-grown, bioavailable forms |
I chose Wild Nutrition specifically because their fertility supplement uses food-grown nutrients — meaning the vitamins and minerals are bound to food matrices for better absorption. I still recommend it to clients today.
Finding the right supplement was its own journey. I tried three different prenatals before Wild Nutrition. Most use synthetic nutrient forms — folic acid instead of methylfolate, cyanocobalamin instead of methylcobalamin. Up to 40% of people have MTHFR gene variations that make converting these synthetic forms inefficient. Wild Nutrition sidesteps the problem with food-grown nutrients bound to food matrices for better absorption. It's not a sponsorship — I genuinely believe it's the best option I've found, and it's what I recommend to every client.
⏰ Start Earlier Than You Think
Most fertility advice focuses on a 3-month window before conception. I think that's too late. Egg development takes approximately 90 days — but the nutritional and hormonal environment those eggs develop in benefits from a much longer runway. I started my protocol 14 months before I conceived. If you're reading this and thinking about trying in the next year or two, start now.
The Results: AMH 3 → 6.43
I committed to this protocol completely — not for weeks, but for years. And in January 2023, roughly two to three years after my initial test, I had my AMH retested.
The result: 6.43 pmol/L. More than double my original reading.
In a metric that the medical establishment broadly considers unlikely to increase, my levels had risen. Now, I want to be honest about this — there's debate in the scientific community about whether AMH can truly be "raised" through lifestyle interventions, or whether my increase reflects natural fluctuation, better testing conditions, or other variables. I can't prove causation.
But what I can say is this: whether or not the number itself was directly caused by my protocol, what is not debatable is that you can do everything in your power to improve the quality of the eggs you do have. And egg quality — not quantity — is what determines whether a pregnancy is viable.
I almost didn't get retested. Part of me was terrified that the number would be even lower — that all the work, all the changes, all the sacrifice would show up as nothing on a piece of paper. Tim talked me into it. And when the nurse called with the result — 6.43 — I sat on the kitchen floor and cried. Not sad tears this time. Relief. Validation. Proof that my body had been listening.
The Pregnancy — And Why Advocacy Matters
The journey wasn't without setbacks. Before my successful pregnancy, I experienced two chemical pregnancies — early losses before six weeks. Whether those were linked to my low AMH, sperm quality factors, or simply non-viable pregnancies — miscarriage rates sit at around one in four — I'll never know.
The chemical pregnancies were the hardest part of the entire journey. Harder than the diagnosis. Harder than the lifestyle changes. Because for a few days each time, I was pregnant — and then I wasn't. The first one, I told myself it was bad luck. The second, I spiralled. I questioned everything. Was my protocol working? Was my body broken? Tim held me together during those weeks. What got me through was going back to the research — reminding myself that one in four pregnancies ends in early loss, regardless of AMH. That the most common cause is random chromosomal mismatch, not egg quality. Losing an early pregnancy is heartbreaking, but it doesn't mean the next one won't work.
But I kept going. And then I fell pregnant. Properly, fully, beautifully pregnant.
But the story wasn't over. Remember those three LLETZ procedures? My weakened cervix became a live concern during pregnancy. I pushed the NHS for additional monitoring — extra cervical checks that wouldn't have happened without my insistence. For a while, the scans were reassuring. Then the NHS told me I didn't need them anymore.
Tim and I felt uneasy. We pushed back. And it was pure chance that led to a final cervical check by a doctor who was about to leave. My cervix had shortened from 30mm to 15mm. It was too late for a cervical stitch. They prescribed additional progesterone, but both Tim and I believe the monitoring should never have been stopped.
I'd dreamed of a home birth. I'd visualised every detail. But with a short cervix, the consultants were honest: I would almost certainly not make it to term.
Bowie arrived a month early. He was healthy. He was perfect.
And he was proof — not just that low AMH doesn't have to mean the end of your story, but that advocating for yourself during pregnancy can be just as important as everything you do before it.
What You Can Do Right Now
I know this list will feel overwhelming. When I was in your position, every article I read added ten more things to worry about. So let me be clear: you don't have to do everything at once. I didn't. I started with three things — CoQ10, cutting alcohol, and switching to organic for the Dirty Dozen. That was week one. Everything else came gradually over two months. Give yourself grace. The fact that you're reading this, educating yourself, taking action — that already puts you ahead.
If you're reading this with a low AMH result in hand, here's where to start — based on what I did and what I now recommend to clients:
Immediate Actions (This Week)
- Get your full fertility panel — AMH alone isn't enough. Ask for FSH, LH, oestradiol, thyroid function, vitamin D, and an antral follicle count (AFC) ultrasound.
- Start CoQ10 — 200mg/day of ubiquinol form. This is the single supplement with the strongest evidence for egg quality.
- Book a vitamin D test — deficiency is incredibly common and directly linked to fertility outcomes. Aim for 75–100 nmol/L.
First Month
- Clean up your diet — shift towards a Mediterranean pattern. More oily fish, berries, leafy greens, olive oil, nuts. Less sugar, processed food, alcohol.
- Switch to organic for the Dirty Dozen — strawberries, spinach, kale, peaches, apples, grapes at minimum.
- Audit your toxin exposure — swap plastic food containers for glass, check your skincare for parabens and phthalates, ditch synthetic fragrances.
Ongoing
- Move gently — walk, swim, yoga. Stop HIIT and marathon training.
- Sleep 8 hours — non-negotiable. Your body repairs and produces hormones while you sleep.
- Manage stress actively — acupuncture, meditation, journaling, therapy. Cortisol is a fertility killer.
- Be patient — egg development takes ~90 days. Meaningful changes need at least 3–6 months. I gave it 14 months.
Can You Actually Increase Your AMH?
This is the honest section. The scientific community is divided:
The "no" camp says: AMH reflects your remaining follicle pool, which is fixed at birth and declines with age. You can't create new follicles, so AMH can only go down.
The "it's complicated" camp says: AMH measures follicles that are actively developing right now — and the number of follicles recruited in each cycle can be influenced by hormonal environment, inflammation, oxidative stress, and nutritional status. Improving these factors may allow more dormant follicles to activate, temporarily raising AMH.
What the evidence shows:
- DHEA supplementation (75mg/day) for 4+ months improved AMH in women with diminished ovarian reserve in several studies (Gleicher et al., 2011; Narkwichean et al., 2013) — though I didn't take DHEA personally and it should only be used under medical supervision.
- Vitamin D supplementation has been associated with higher AMH levels in deficient women (Dennis et al., 2017).
- My own AMH rose from 3 to 6.43 pmol/L over approximately 2–3 years of protocol adherence.
I'm transparent about this because I believe you deserve honesty, not hype. I can't promise that following my protocol will raise your AMH number. What I can promise is that every element of it is designed to give your existing eggs the best possible chance of developing into healthy, viable embryos. And that's ultimately what matters.
Here's what I've come to believe after living through this and working with hundreds of women since: it doesn't actually matter whether my protocol 'raised' my AMH or whether the increase reflects natural variation. What matters is that during those 14 months, I transformed my health. My cycles were more regular than they'd ever been. My energy was better. My stress was managed. My body was in the best possible state to conceive. Whether that shows up as a higher AMH number or not, the outcome speaks for itself.
When to Consider IVF or Egg Freezing
I walked away from egg freezing — but that doesn't mean it's the wrong choice for everyone. Consider it seriously if:
- Your AMH is very low and your AFC (antral follicle count) is also low
- You're 38+ and not in a position to try to conceive in the next 12 months
- You have other fertility factors beyond low AMH (blocked tubes, severe endometriosis, male factor)
- You've been trying naturally for 6+ months without success (less if you're over 35)
If you do pursue IVF with low AMH, ask your clinic about mini IVF or natural cycle IVF protocols — these use lower doses of stimulation drugs and can be more effective for low responders than standard protocols (Zhang et al., 2016).
And regardless of which path you choose — natural or assisted — optimising your egg quality through nutrition and lifestyle will support your outcome. These approaches aren't mutually exclusive.
💌 A note from Danielle
If I could sit across from every woman who's just received a low AMH result, this is what I'd say: please don't let that number define your future. I had really low levels. They told me a natural pregnancy was unlikely. But I have a beautiful little boy who proves otherwise. Focus on quality. The stronger and healthier your eggs are, the better your chances. And you have far more control over that than anyone's telling you. I built Fertilitys so that no woman has to navigate this alone — and everything I've shared in this article is exactly what I'd tell you if you were sitting in my kitchen right now.

Danielle Bowen MSc, RNutr
Registered Nutritionist & Fertility Specialist
I was diagnosed with an AMH of 3 pmol/L at 32. I built a science-backed protocol that raised my levels to 6.43 and led to the natural conception of my son Bowie. I now help other women optimise their fertility through evidence-based nutrition and lifestyle strategies.
The Bottom Line
A low AMH result is frightening. I know because I've been there — staring at a number that felt like it meant the end of something before it even started.
But here's what I want you to take away:
- AMH measures quantity, not quality — and quality is what makes a baby
- Research shows AMH is a poor predictor of natural conception
- You have far more control over egg quality than most clinics suggest
- Start your protocol at least a year before you want to conceive — not three months
- Advocate for yourself — push for the full picture, the extra tests, the monitoring you deserve
I was told at 32 that a natural pregnancy was unlikely. I was told nutrition couldn't help. I was told my only option was £15,000+ of egg freezing with poor odds.
I have a beautiful boy called Bowie who proves otherwise.
If my story has taught me anything, it's this: please don't let that number define your future. A low AMH is not a sentence. It's not an indication that you can't get pregnant. Focus on quality. Do everything in your power. And know that you have far more agency in this than anyone's telling you.
Frequently Asked Questions
References
- Dewailly D, et al. (2014). The physiology and clinical utility of anti-Müllerian hormone in women. Human Reproduction Update, 20(3), 370-385. DOI
- Broer SL, et al. (2014). AMH: the holy grail of ovarian reserve testing? Human Reproduction, 29(12), 2637-2638. PubMed
- Tal R & Seifer DB (2017). Ovarian reserve testing: a user’s guide. American Journal of Obstetrics and Gynecology, 217(2), 129-140. DOI
▸Can you get pregnant naturally with low AMH?
Yes — and the research supports this clearly. A 2017 JAMA study of 750 women found no significant difference in natural pregnancy rates between women with low AMH and those with normal levels (Steiner et al., 2017). I conceived naturally with an AMH of approximately 6.43 pmol/L (originally 3). AMH predicts IVF response, not natural fertility.
▸What is considered a dangerously low AMH level?
An AMH below 3.5 pmol/L (0.5 ng/mL) is generally considered very low, but 'dangerous' is misleading — AMH isn't a health risk marker, it's a fertility indicator. Even very low levels don't mean pregnancy is impossible. My AMH was 3 pmol/L (0.42 ng/mL) when I was diagnosed, and I went on to conceive naturally.
▸Can diet and lifestyle actually increase AMH?
The My AMH doubled from 3 to 6.43 pmol/L during the twelve months I followed this protocol. I changed my diet, my supplements, my lifestyle, and my stress levels simultaneously — and the research behind every element is solid. Vitamin D supplementation has been directly associated with higher AMH in deficient women (Dennis et al., 2017), and every other component of my protocol has peer-reviewed evidence supporting its effect on egg quality and ovarian function.
▸How long does it take to improve egg quality with low AMH?
Egg development takes approximately 90 days from dormant follicle to ovulation-ready oocyte. Any intervention needs at least 3 months to affect the eggs you'll ovulate. I recommend a minimum of 6 months, and ideally starting your protocol a full year before you want to conceive. I started mine 14 months before Bowie was conceived.
▸Should I freeze my eggs if my AMH is low?
It depends on your full picture — not just AMH. Consider egg freezing if your AFC is also low, you're 38+, you can't try to conceive soon, or you have other fertility factors. But know that low AMH often means fewer eggs per retrieval cycle, which may require multiple rounds. I chose not to freeze mine, but it's a personal decision.
▸What supplements should I take for low AMH?
Based on my protocol and the current evidence: CoQ10 (200mg/day ubiquinol form), vitamin D (test first, aim for 75–100 nmol/L), omega-3 (EPA/DHA from fish oil or algae), and a high-quality prenatal with methylfolate. I use Wild Nutrition's fertility supplement. Some women also benefit from DHEA under medical supervision.
▸Is low AMH the same as early menopause?
No. Low AMH means you have fewer developing follicles than average — it doesn't mean menopause is imminent. Women with low AMH can still have regular menstrual cycles and ovulate normally for years. Premature ovarian insufficiency (POI) is a separate diagnosis involving additional criteria beyond AMH alone.
▸Is low AMH the same as infertility?
No. Low AMH indicates reduced ovarian reserve (fewer eggs remaining), not infertility. Many women with low AMH conceive naturally. It does suggest that your fertile window may be shorter over your lifetime, making timing and proactive planning more important.
▸What AMH is considered low?
Generally, AMH below 1.0 ng/mL (7.0 pmol/L) is considered low for reproductive-age women. Below 0.5 ng/mL is very low. However, context matters — a 'low' AMH for a 28-year-old is different from a 'low' AMH for a 42-year-old.
▸Should I freeze my eggs if my AMH is low?
This depends on your age, life situation, and how low your AMH is. Egg freezing with low AMH may require multiple cycles to collect enough eggs. Discuss with a fertility specialist — they can model expected outcomes based on your specific numbers.
You might also find helpful:
References
- Steiner AZ, Pritchard D, Stanczyk FZ, et al. Association between biomarkers of ovarian reserve and infertility among older women of reproductive age. JAMA. 2017;318(14):1367–1376.
- Li HWR, Lee VCY, Lau EYL, et al. Role of baseline antral follicle count and anti-Müllerian hormone in prediction of cumulative live birth in the first in vitro fertilisation cycle. Frontiers in Endocrinology. 2021;12:675390.
- Iliodromiti S, Kelsey TW, Wu O, et al. The predictive accuracy of anti-Müllerian hormone for live birth after assisted conception. Human Reproduction Update. 2014;20(4):560–570.
- Ben-Meir A, Burstein E, Borber A, et al. Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell. 2015;14(5):887–895.
- Baudry J, Assmann KE, Touvier M, et al. Association of frequency of organic food consumption with cancer risk. JAMA Internal Medicine. 2018;178(12):1597–1606.
- Chiu YH, Williams PL, Gillman MW, et al. Association between pesticide residue intake from consumption of fruits and vegetables and pregnancy outcomes among women undergoing infertility treatment. JAMA Internal Medicine. 2018;178(1):17–26.
- Karayiannis D, Kontogianni MD, Mendorou C, et al. Adherence to the Mediterranean diet and IVF success rate among non-obese women attempting fertility. Human Reproduction. 2018;33(3):494–502.
- Gaskins AJ, Chavarro JE. Diet and fertility: a review. American Journal of Obstetrics and Gynecology. 2018;218(4):379–389.
- Chu J, Gallos I, Tobias A, et al. Vitamin D and assisted reproductive treatment outcome. Human Reproduction. 2018;33(1):65–80.
- Dennis NA, Houghton LA, Jones GT, et al. The level of serum anti-Müllerian hormone correlates with vitamin D status in men and women but not in boys. Journal of Clinical Endocrinology & Metabolism. 2012;97(7):2450–2455.
- Fan D, Liu L, Xia Q, et al. Female alcohol consumption and fecundability: a systematic review and dose-response meta-analysis. Scientific Reports. 2017;7:13815.
- Gleicher N, Weghofer A, Barad DH. Dehydroepiandrosterone (DHEA) reduces embryo aneuploidy: direct evidence from preimplantation genetic screening. Reproductive Biology and Endocrinology. 2010;8:140.
- Zhang JJ, Merhi Z, Hassan N, et al. Minimal stimulation IVF versus conventional IVF: a randomized controlled trial. American Journal of Obstetrics and Gynecology. 2016;214(1):96.e1–96.e8.
- Clifford T, Howatson G, West DJ, et al. The potential benefits of red beetroot supplementation in health and disease. Nutrients. 2015;7(4):2801–2822.
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. AMH results should be interpreted by a qualified healthcare professional in the context of your full fertility assessment. Always consult your doctor before starting any supplement protocol.
⚕️ Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making decisions about your fertility or reproductive health.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











