Endometriosis and Fertility: What You Need to Know
Your complete guide to endometriosis and getting pregnant — from a fertility nutritionist who believes in evidence, advocacy, and never giving up hope.


Yes, you can get pregnant with endometriosis. Around 60–70% of women with endometriosis conceive naturally or with treatment. Laparoscopic excision surgery improves pregnancy rates by up to 43%, and there's a well-documented "golden window" of 6–12 months after surgery where fertility is at its highest. The condition affects around 10% of women — but a diagnosis is not a sentence.
Key Takeaways
- Endometriosis affects roughly 1 in 10 women, and around 30–50% of those will experience some degree of fertility difficulty — but the majority still conceive
- Stage doesn't equal severity. Some women with stage 4 have no symptoms and get pregnant quickly, while stage 1 can cause significant pain and delay
- Excision surgery (not ablation) is the gold standard, and the 6–12 months after surgery is your best window to try
- Silent endometriosis — endo with zero classic symptoms — is behind roughly 30% of unexplained infertility cases
- An anti-inflammatory diet, targeted supplements like CoQ10 and omega-3, and working with an endo-specialist surgeon can all meaningfully improve your chances
If you've just been told you have endometriosis, I know exactly where your mind went first. Not to the pain management plan. Not to the surgery options. Straight to: can I still have a baby?
That question lands like a punch. And the fear it brings — this deep, rushing dread that something has been quietly stealing your fertility while doctors spent years telling you your pain was normal — is one of the most common things I hear from women who reach out to me.
So let me say this clearly, right at the top: endometriosis and fertility are not mutually exclusive. Most women with endo go on to conceive. Some need help, some need surgery, some need time and patience — but the statistics are firmly on your side, even if it doesn't feel that way right now.
This guide walks through exactly how endometriosis affects your ability to get pregnant, what the research actually shows about your chances at every stage, why surgery timing matters more than most doctors explain, and what you can do right now — nutritionally, practically, emotionally — to give yourself the strongest possible foundation.
What Is Endometriosis?
Endometriosis is a condition where tissue similar to the lining of the uterus grows outside it — on the ovaries, fallopian tubes, bowel, bladder, and sometimes further. This tissue responds to your menstrual hormones just like your uterine lining does: it thickens, breaks down, and bleeds each cycle. But because it has nowhere to go, it triggers chronic inflammation, adhesions (internal scarring), and pain that can range from mild to completely debilitating.
It affects approximately 10% of reproductive-age women worldwide — around 190 million people, according to the WHO. And here's the part that makes me genuinely angry: the average time from first symptoms to confirmed diagnosis is 6.7 years (Boujenah et al., 2025). Over 65% of women are initially misdiagnosed. Years of being told your period pain is "normal" or that you're being dramatic. Years where the condition can quietly progress.
The ASRM (American Society for Reproductive Medicine) classifies endometriosis into four stages based on the number, size, and depth of lesions:
- Stage I (Minimal): Small, superficial implants
- Stage II (Mild): More and slightly deeper implants
- Stage III (Moderate): Deep implants, small cysts on one or both ovaries, some adhesions
- Stage IV (Severe): Deep implants, large cysts (endometriomas), dense adhesions
But — and this is critical — your stage doesn't necessarily predict your symptoms or your fertility. Some women with stage 4 feel nothing and conceive within months. Some with stage 1 are in daily agony and struggle for years. What matters more is where the endometriosis is growing and whether it's caused structural damage (Pascoal et al., 2020).
How Endometriosis Affects Your Fertility
Endometriosis doesn't cause infertility through a single mechanism. It attacks on multiple fronts, which is partly why it's so unpredictable — and partly why treatment needs to be equally multi-layered.
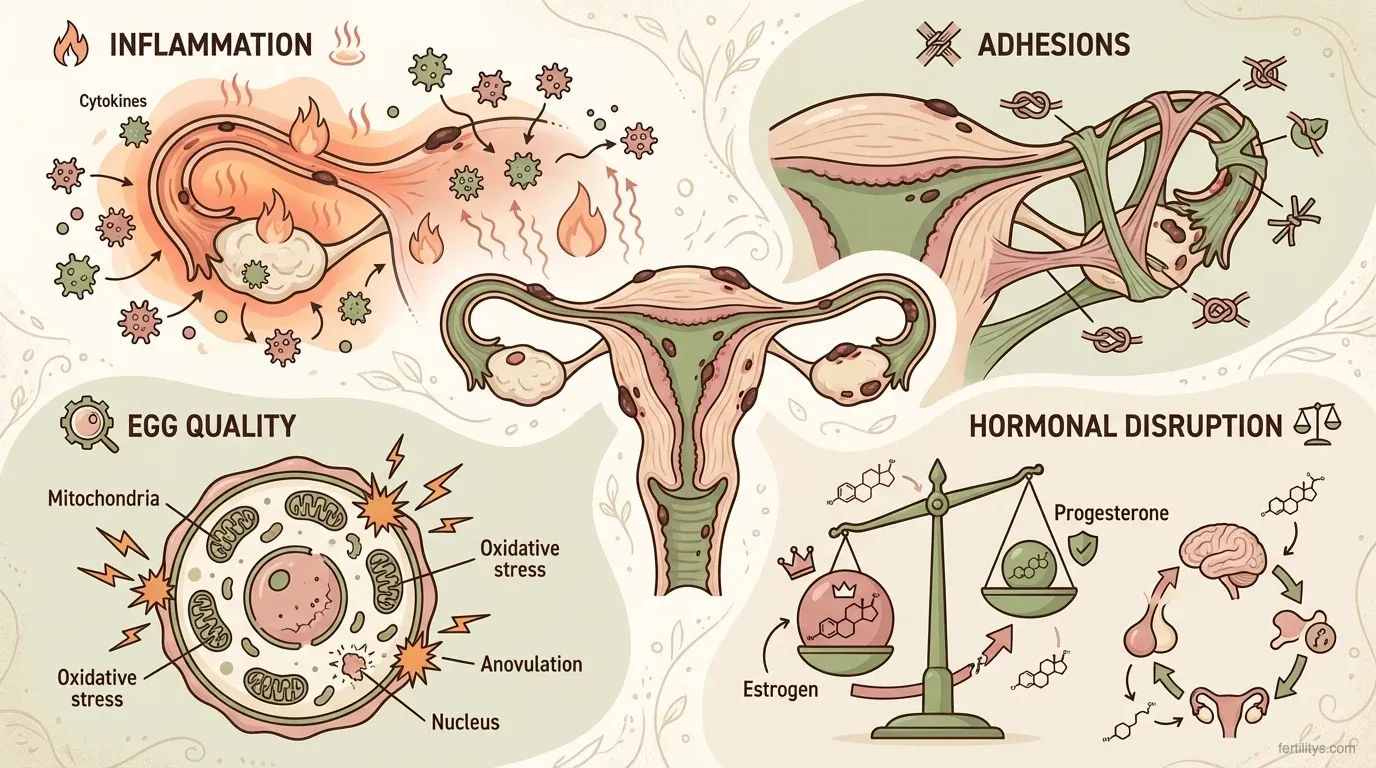
Inflammation and the Pelvic Environment
The most significant factor for many women. Endometrial lesions create a chronically inflamed environment in the pelvis, flooding the area with cytokines, chemokines, and immune cells that are hostile to sperm, eggs, and embryos. This inflammation can prevent implantation even when everything else looks textbook — ovulation is happening, tubes are open, sperm is healthy (Chen et al., 2025).
Adhesions and Structural Damage
As endometriosis progresses, the body forms adhesions — bands of scar tissue that can stick organs together, distort the fallopian tubes, or block them entirely. If both ovaries develop endometriomas (blood-filled cysts) and become adhered to the pelvic sidewall, ovulation itself can be physically obstructed.
Egg Quality and Ovarian Reserve
There's growing evidence that endometriosis contributes to oxidative stress within the ovaries, which can damage oocytes and reduce their quality. Impaired mitochondrial function, dysregulated lipid metabolism, and iron-induced free radical damage all play a role (Chen et al., 2025). This matters even in early-stage disease. If you're concerned about your ovarian reserve, an AMH test can give you a baseline — though remember that AMH measures quantity, not quality.
Hormonal Disruption
Endometriosis can dysregulate both the hypothalamic-pituitary-ovarian axis (your core reproductive hormone signalling) and the HPA axis (your stress response system). The result: altered gonadotropin secretion, elevated cortisol and prolactin, and a hormonal environment that's less conducive to conception. This is one reason why stress management and cycle syncing can be genuinely helpful alongside medical treatment — not as replacements for it, but as part of the bigger picture.
Can You Get Pregnant with Endometriosis?
Yes. The majority of women with endometriosis do get pregnant, and I want to put real numbers behind that because vague reassurance isn't what you need right now.
Normal monthly fecundity (the chance of conceiving in any given cycle) sits at 15–20% for couples without fertility issues. For women with untreated endometriosis, that drops to roughly 2–10% per cycle — lower, but not zero. And that's untreated. With appropriate surgical or medical intervention, the picture changes substantially.
A 2024 meta-analysis found that laparoscopic surgery for stage I–II endometriosis increased the live birth rate by 52% compared to no surgical treatment (relative risk 1.52, 95% CI: 1.26–1.84). For more advanced disease (stage III–IV), spontaneous pregnancy rates jumped from 4% pre-surgery to 43% post-surgery in one large series of 216 women (Leonardi et al., 2024).
The overall one-year postoperative pregnancy rate across all stages is around 57%, with a live birth rate of nearly 52%. And up to 59% of those pregnancies happen naturally — no IVF required.
Here's something else the data shows that often gets lost in the fear: the 2022 HFEA database study covering 13,614 IVF cycles in women with endometriosis found no significant difference in live birth rates compared to women without endo. When endo is treated, IVF outcomes are comparable (Raperport et al., 2022).
None of this is to minimise how hard the journey can be. But the evidence is clear: endometriosis does not mean you can't have a baby.
Silent Endometriosis and Unexplained Infertility
This is the section I wish every GP in the country would read.
Around 20–25% of women with endometriosis have no classic symptoms at all — no painful periods, no pelvic pain, no bloating, no pain during sex. They have what's called "silent" endometriosis. And they often only discover it after months or years of trying to conceive, when all the standard fertility tests come back normal and they're labelled with "unexplained infertility."
Research shows that roughly 30% of women with unexplained infertility are eventually diagnosed with endometriosis on laparoscopy (Tsamantioti et al., 2023). In one study, 39% of asymptomatic, apparently fertile women who had laparoscopy for other reasons were found to have endometriosis.
If you've been trying to conceive for 12+ months with no obvious cause, and your blood work, scans, and partner's semen analysis all look fine — push for a conversation about diagnostic laparoscopy. It's the only way to definitively confirm or rule out endometriosis. Ultrasound can pick up endometriomas and deep infiltrating disease, but it misses superficial peritoneal endometriosis completely.
This isn't about creating anxiety where there's none needed. It's about making sure something treatable isn't being overlooked.
Endometriosis Surgery and the "Golden Window" for Getting Pregnant
If you're weighing up whether to have endometriosis surgery before trying to conceive (or before IVF), the research is firmly in favour of it for most women.
Excision vs. Ablation
Not all endometriosis surgery is equal. There are two main approaches:
Excision cuts the endometrial lesion out completely — below the surface, removing the root. Think of it as digging out a weed. Ablation burns or lasers the surface of the lesion, destroying what's visible but potentially leaving deeper tissue behind.
Excision is considered the gold standard. It reduces inflammatory cytokine levels more effectively, has lower recurrence rates for deep disease, and is associated with better fertility outcomes — particularly for ovarian endometriomas (RCOG Guideline No. 24). The Endocan trial (n=341) found that women who had excision or ablation had a pregnancy rate of 30% compared to 17% for diagnostic laparoscopy alone, with excision showing particular benefit for more advanced disease.
If you're being offered surgery, ask your surgeon directly: "Do you excise or ablate?" And if they ablate, consider seeking a referral to a specialist endometriosis centre. NICE guideline NG73 recommends that complex endometriosis should be managed in specialist services with advanced laparoscopic skills.
The Golden Window
After laparoscopic excision, there's a well-recognised 6–12 month window where fertility is significantly enhanced. Inflammation is at its lowest, adhesions have been cleared, and the pelvic environment is the most hospitable it's likely to be. This is your best shot at natural conception.
The data backs this up consistently. The one-year postoperative pregnancy rate is approximately 57% (Leonardi et al., 2024). Many women in the research conceived within the first 3–6 months. After 12 months, endometriosis can begin to recur, so timing matters.
If you're planning surgery, talk to your surgeon and your fertility team about having a conception plan ready for recovery. Don't waste the window with logistics.
IVF, IUI, and Endometriosis: What You Need to Know
Not everyone needs IVF. But for some women with endometriosis — particularly those with bilateral endometriomas, tubal damage, or other coexisting factors like male factor infertility — assisted reproduction is the right path.
IUI (intrauterine insemination) can improve fertility in minimal to mild endometriosis (RCOG Guideline No. 24). It's less invasive, less expensive, and worth considering as a first step before IVF — especially if your tubes are patent and your partner's sperm is healthy. Our IUI vs IVF comparison breaks down costs, success rates, and how to decide.
IVF outcomes with endometriosis depend heavily on whether the disease has been treated. A striking finding: untreated endometriosis gives a live birth rate of around 28%, while treated endometriosis reaches 44–46% — comparable to women without endo (Raperport et al., 2022). Specialised endometriosis IVF programmes report 10–15% higher live birth rates than the national average.
If you're considering IVF, discuss surgical treatment first with your consultant. For many women, excision before IVF transfer — rather than skipping straight to egg retrieval — produces better outcomes.
Does Endometriosis Increase Miscarriage Risk?
This is something women worry about deeply but rarely get a straight answer on, so here it is: endometriosis is associated with a modestly increased risk of miscarriage, but the increase is smaller than many people fear.
A large nationwide cohort study found that women with endometriosis had a slightly higher rate of pregnancy loss — particularly recurrent loss (3+ miscarriages), where the odds ratio was 1.44 compared to controls (Kvaskoff et al., 2022). The general miscarriage rate in women with endo sits around 20% versus 12% in controls.
Two important caveats. First, for women undergoing IVF, endometriosis does not appear to increase miscarriage risk — likely because of the egg selection process and controlled hormonal support. Second, much of the elevated risk may be driven by coexisting conditions rather than endometriosis alone.
The biggest co-factor is adenomyosis — a related condition where endometrial-like tissue grows into the muscular wall of the uterus. Around 65–70% of women with endometriosis also have adenomyosis, and it's adenomyosis that carries the stronger miscarriage association (31% miscarriage rate vs. 14% without it). If you have endo and are concerned about pregnancy loss, ask your consultant specifically about adenomyosis screening.
For more on miscarriage statistics and what the week-by-week data actually shows, see our miscarriage risk by week guide.
What You Can Do Right Now to Support Your Fertility with Endometriosis
Beyond surgery and medical treatment, there are evidence-based nutritional and lifestyle strategies that can genuinely help. This isn't about replacing medical care — it's about building the strongest possible biological foundation alongside it.
Follow an Anti-Inflammatory Diet
Endometriosis is fundamentally an inflammatory condition, and your diet directly influences the inflammatory environment in your pelvis. Research consistently links a Mediterranean-style, anti-inflammatory diet with reduced endometriosis symptoms — less pain, less bloating (goodbye, endo belly), and improved gastrointestinal function (Nirgianakis et al., 2022).
Focus on: oily fish (salmon, mackerel, sardines), colourful vegetables and berries, nuts and seeds, olive oil, whole grains, and quality protein. Reduce: processed foods, refined sugar, red meat, trans fats, and alcohol. It doesn't need to be perfect. It needs to be consistent.
We've got a full rundown of the best fertility foods if you want specific meal ideas.

Supplements Worth Discussing with Your Doctor
Several supplements have emerging evidence specifically for endometriosis and fertility:
- CoQ10 — Supports mitochondrial energy production in eggs. Meta-analyses show it increases clinical pregnancy rates in ART. CoQ10 levels decline after 30, making supplementation particularly relevant if you're mid-thirties or older.
- Omega-3 fatty acids — Anti-inflammatory, improves folliculogenesis and oocyte quality. A combined omega-3 and alpha-lipoic acid protocol also reduced endo-related pain in clinical trials.
- N-acetylcysteine (NAC) — A powerful antioxidant that has been shown to reduce endometrioma size and lower CA-125 levels. Two prospective studies found pregnancy rates of 75–86% in women taking NAC alongside standard care — striking numbers, though larger trials are still needed.
- Vitamin D — Deficiency is both a risk factor for endometriosis and independently associated with reduced fertility. Supplementation has been shown to improve endo-related pain. The NHS recommends 10mcg daily for everyone in the UK, and your fertility consultant may suggest more.
Always discuss supplements with your doctor before starting them, especially if you're also taking hormonal medication for endometriosis management.
Manage Stress — Seriously
I know "manage your stress" can feel like the most unhelpful advice on earth when you're dealing with chronic pain, fertility anxiety, and a 6-year diagnostic delay. But the HPA axis disruption that endometriosis causes means your cortisol and prolactin levels may already be elevated, and chronic stress compounds that.
Gentle yoga, breathing work, walking in nature, acupuncture, and therapy aren't luxuries — they're tools that directly influence your hormonal environment. And if the emotional weight of all this feels unbearable, our fertility anxiety guide has practical strategies that go beyond "just relax."

The Bottom Line
Endometriosis can make getting pregnant harder. It's not always straightforward, and I won't pretend the journey isn't exhausting sometimes — emotionally, physically, financially. The diagnostic delays are appalling. The dismissiveness from some healthcare providers is real. And the fear that comes with hearing the word "endometriosis" in the same sentence as "fertility" is completely valid.
But the evidence tells a story of genuine hope. The majority of women with endometriosis conceive — many naturally, many after surgery, and many with assisted reproduction. Excision surgery opens a golden window. Anti-inflammatory nutrition and targeted supplements support your body from the inside. And advocating for yourself — pushing for the right surgeon, the right investigations, the right timing — can make all the difference.
You are not broken. You have a treatable condition. And the statistics are better than you think.
Frequently Asked Questions
Can you get pregnant naturally with stage 4 endometriosis?
Yes. While stage 4 is classified as "severe," staging doesn't reliably predict fertility. Many women with stage 4 endometriosis conceive naturally — particularly after excision surgery, which can increase spontaneous pregnancy rates from around 4% to over 40%. The location of the endometriosis and whether it's caused structural damage matters more than the stage number alone.
How long after endometriosis surgery should I try to conceive?
As soon as you've recovered from the procedure — typically 2–4 weeks for laparoscopic surgery. The "golden window" of enhanced fertility lasts roughly 6–12 months after excision, so most specialists recommend trying during this period. After 12 months, endometriosis can begin to recur. Have a conception plan ready before surgery so you can act quickly during recovery.
Does endometriosis get worse with age?
Endometriosis can progress over time, though it doesn't always. The condition is oestrogen-dependent, so it typically remains active throughout your reproductive years and often improves after menopause. Delaying diagnosis and treatment gives the disease more time to cause adhesions and structural damage, which is one reason early investigation matters — especially if you're planning a pregnancy.
Should I do IVF or surgery first?
It depends on your individual situation, but emerging evidence favours excision surgery before IVF transfer for many women. Treated endometriosis gives IVF live birth rates of 44–46% compared to 28% when untreated. Discuss both options with your fertility specialist and consider seeking a second opinion from an endometriosis centre if surgery isn't being offered.
What is silent endometriosis?
Silent endometriosis is endometriosis that causes no noticeable symptoms — no painful periods, no pelvic pain, no bloating. Around 20–25% of women with endo are asymptomatic. It's often only discovered during investigation for infertility or during surgery for another reason. Roughly 30% of "unexplained infertility" cases are later found to be caused by silent endometriosis.
Can diet cure endometriosis?
Diet cannot cure endometriosis, and anyone claiming it can is overstating the evidence. What an anti-inflammatory diet can do is reduce symptoms (pain, bloating, fatigue), lower systemic inflammation, and create a more favourable environment for conception. Think of it as one important layer of a multi-layered approach — alongside medical treatment, surgery where appropriate, and targeted supplementation.
References
- World Health Organization. (2023). Endometriosis Fact Sheet. WHO.
- Boujenah, J. et al. (2025). Factors contributing to the delayed diagnosis of endometriosis — a systematic review and meta-analysis. Frontiers in Medicine. DOI
- Chen, Y. et al. (2025). Update on the pathogenesis of endometriosis-related infertility based on contemporary evidence. PubMed. PMID: 40130159
- Tsamantioti, E. et al. (2023). Epidemiology of infertility in women with endometriosis. PubMed. PMID: 38183767
- Pascoal, E. et al. (2020). Classification of endometriosis. PMC. PMC7787892
- Leonardi, M. et al. (2024). The Impact of Laparoscopic Surgery on Fertility Outcomes in Patients with Minimal/Mild Endometriosis. PMC. PMC11355624
- RCOG. Green-top Guideline No. 24: Endometriosis, Investigation and Management.
- NICE. (2024). NG73: Endometriosis — diagnosis and management. Updated November 2024.
- Raperport, C. et al. (2022). Endometriosis and IVF treatment outcomes: unpacking the process. PMC. PMC10629090
- Kvaskoff, M. et al. (2022). Endometriosis is associated with pregnancy loss: a nationwide historical cohort study. Fertility and Sterility. Full text
- Nirgianakis, K. et al. (2022). Anti-Inflammatory Diets in Fertility: An Evidence Review. PMC. PMC9570802
- Porpora, M.G. et al. (2022). Dietary supplements for treatment of endometriosis: A review. PMC. PMC8972862
Cite This Page
Bowen, D. (2026). Endometriosis and Fertility: What You Need to Know. Fertilitys. Retrieved from https://www.fertilitys.com/fertility-treatments/endometriosis-and-fertility/
Medical Disclaimer: This article is written by a registered nutritionist (ANutr) and is intended for informational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider before making changes to your diet, supplement routine, or treatment plan. If you're experiencing symptoms of endometriosis or difficulty conceiving, please speak with your GP or a fertility specialist.
Written by

Subscribe to Fertilitys
All my Free Resources. No spam. Unsubscribe anytime.











